

Copyrights: Mujtaba Shuja, Sarah Islamie Farsani, Hamid Salehiniya, Salman Khazaei, Mahdi Mohammadian, Mohammad Aryaie, Pezhman Bagheri, Fatemeh Allah Bakeshei, Abdollah Mohammadian-Hafshejani, 2017. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: Liver Cancer (LC) is one of the most common cancers in the worldwide. This cancer is considered as the fifth most common cancer in male and the ninth most common cancer in female. However, socioeconomic factors and morbidity and mortality of cancer are linked by sophisticated and flexible pathways. We were investigated the association between incidence and mortality of LC with the Human Development Index (HDI) in European countries in 2012. Methods: This study was an ecologic study in European countries for assessment the correlation between Age-Specific Incidence Rate (ASIR) and Age-Specific Mortality Rate (ASMR) of LC with HDI and its details including: Life expectancy at birth, Mean years of schooling and Gross National Income (GNI) per capita. We used of Pearson correlation method for appraisement the association between HDI and its components with ASIR and ASMR. Data of study was analyzed by SPSS15 statistical analysis software; the significance level of the tests was considered P˂0.05. Results: Generally in 2012, European countries have recorded 63,462 new cases of LC, crude rate was 8.6 and ASIR was 4.3 per 100,000. On the other hand in Europe countries in 2012, 62,191 cases of deaths were occurred due to LC, crude rate was 8.4 and ASMR was 3.9 per 100,000. Strong positive Correlation was observed between ASIR and ASMR (r = 0.848; P ≤ 0.001). HDI have weak negative correlation with ASIR of LC (r = - 0.194; P = 0.230), and strong negative correlation with ASMR of LC(r= - 0.515; P = 0.001). Conclusion: Increase in the human development index was associated with reduce in incidence and mortality of LC.
Introduction
Liver cancer (LC) is one of the most common cancers in the worldwide Wei et al., 2014. This cancer is considered as the fifth most common cancer in male and the ninth most common cancer in female Hall and Wild, 2003. Estimates from the year 2012 indicate that 782,451 new cases of LC occurred worldwide, including 554,369 cases in male and 228,082 cases in female. Also in this year, 745533 case of death of LC were observed in worldwide, including 521,041 cases in male and 224,492 cases in female Ferlay et al., 2014. This tumor accounted for 5.6% of all human cancers (7.5% among male and 3.5% among female) in Ferlay et al., 2001.
In the worldwide, the areas with high Age Standardized Incidence Rate (ASIR per 100,000) of LC are located in Eastern Asia (ASIR= 20.9), Intermediate rates happen in Africa (ASIR= 8.9) and Middle Africa America (ASIR= 8) and the lowest rates are in South-Central Asia (ASIR= 2.9) and Northern Europe (ASIR= 3.1) Ferlay et al., 2014.
In the Europe, ASIR for LC in 2012 was equal to 4.3 per 100,000, with ranges from a relatively low rate in the Netherlands (ASIR=1.6) to the high rates in Republic of Moldova (ASIR=8.5). Also, Age Standardized Mortality Rate (ASMR per 100,000) for this cancer in the Europe in 2012 was 3.9 per 100,000, with ranges from a relatively low rate in Norway (ASMR=1.7) to the high rates in Republic of Moldova (ASMR=9.5) Mohammadian et al., 2015. LC is ordinarily a problem of the less developed countries Ferlay et al., 2014. Extra than 85% of LC new cases take place in developing countries which do not have suitable detection and treatment services Ferlay et al., 2010. LC is the second most common cause of mortality from cancer in worldwide, estimated to be responsible for closely 746,000 deaths in 2012 (9.1% of the whole death of cancer). The prognosis for LC is very low, so general ratio of LC mortality to incidence is around 0.95 Ferlay et al., 2014.
Socioeconomic factors are connected with cancer incidence and mortality by intricate and variable pathways. One of the most important known meters of socioeconomic factors is Human Development Index (HDI). According to HDI, countries are assigned into four categories: countries with low HDI (HDI≤0.5), countries with Medium HDI (0.8> HDI>0.5), countries with high HDI (HDI≥0.8) and countries with very high HDI (HDI≥0.9) Bray et al., 2012.
In the study that conducted in Asian countries about relationship of incidence and mortality of LC with HDI, negative correlation was observed between ASIR and ASMR with HDI, But this relationships wasn’t significant Mohammadian et al., 2015. Similarly, relationship of HDI and incidence and mortality from other cancers were examined in other studies Ghoncheh et al., 2015Hassanipour-Azgomi et al., 2016Mohammadian et al., 2015Pakzad et al., 2015a, bPakzad et al., 2016Pakzad et al., 2015cRafiemanesh et al., 2015. However, according to our information, no study has been done still regarding the association between the ASIR and ASMR of LC with HDI in European countries; therefore in this study we investigate the association between incidence and mortality of LC with HDI in European countries in 2012.
Materials - Methods
This study was an ecologic study in European countries for appraisal the relationship among Age-Specific Incidence Rate (ASIR) and Age-Specific Mortality Rate (ASMR) with Human Development Index (HDI) and its details including: Life expectancy at birth, average years of schooling and Gross National Income (GNI) per capita. Data about the ASIR and ASMR for every European countries for year 2012 had gathered from GLOBOCAN project that is available in (http://globocan.iarc.fr/Default. aspx) Ferlay et al., 2015. Also data about Human Development Index had extracted from Human Development Report 2013 Malik, 2013.
Details of Methods for estimate the Age-specific incidence rate (ASIR) and Age-specific mortality rate (ASMR) in GLOBOCAN project have been provided in previous reports Ferlay et al., 2010Ferlay et al., 2015Foulkes and Cooney, 2010Pakzad et al., 2015bPakzad et al., 2016.
Statistical analysis
In current report, we used of Pearson correlation method for assessment of correlation between Age-specific incidence rate and Age-specific mortality rate of LC by human development index and its details. All reported ASIR and ASMR were per 100,000. Statistical significance was considered as P<0.05. All P-values reported in study are two-sided. Also, Statistical analyses were performed using SPSS (Version 16.0, SPSS Inc.).
Results
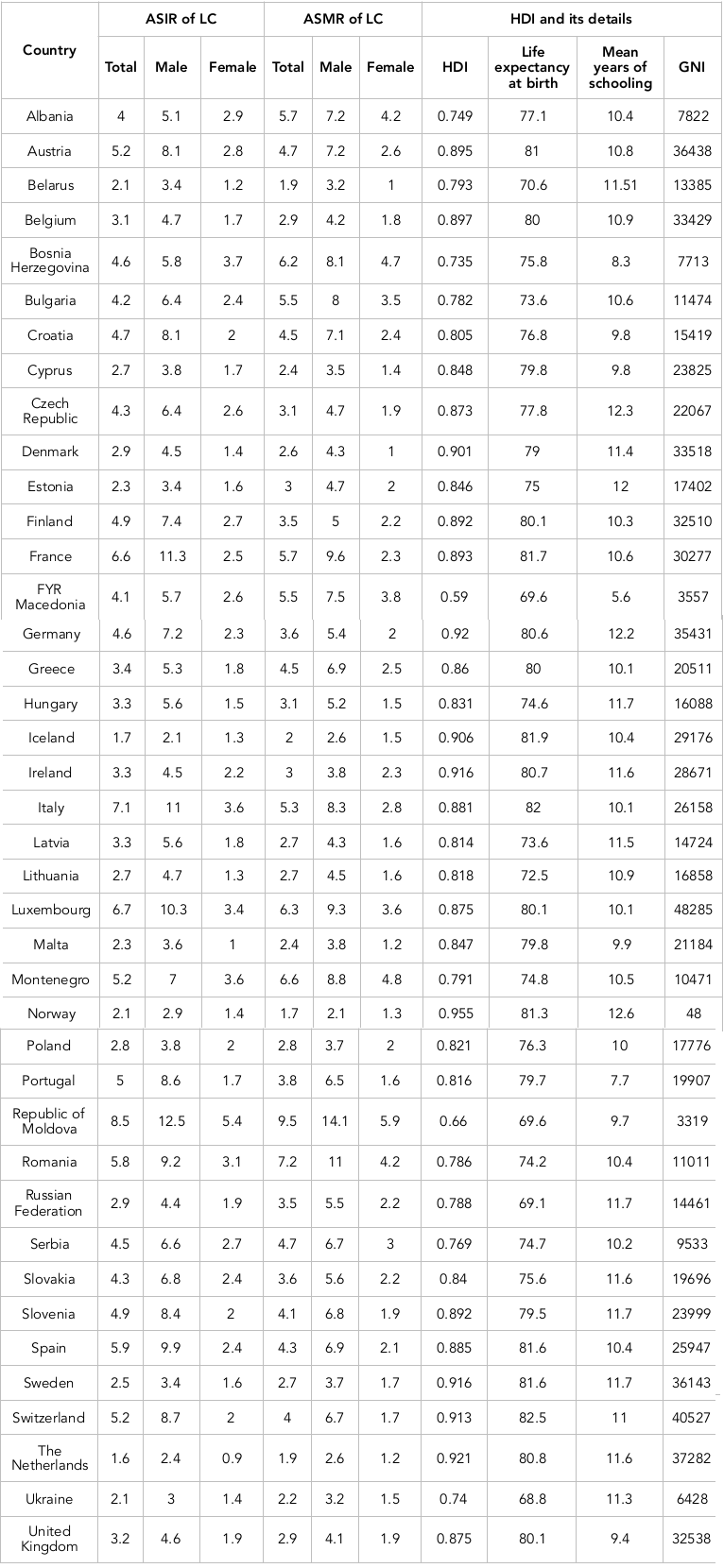
Overall, European countries have recorded 63,462 cases of LC, Crude Rate was 8.6 and ASIR was 4.3 per 100,000. The five countries with the highest ASIR of the LC were Republic of Moldova (ASIR=8.5), Italy (ASIR=7.1), Luxembourg (ASIR=6.7), France (ASIR=6.6), and Spain (ASIR=5.9), respectively. Also, five countries with the lowest ASIR of the LC were The Netherlands (ASIR=1.6), Iceland (ASIR=1.7), Norway (ASIR=2.1), Belarus (ASIR=2.1), and Ukraine (ASIR=2.1), respectively.
On the other hand in Europe countries in 2012, 62,191 cases of deaths occurred due to LC, Crude Rate was 8.4 and ASMR was 3.9 per 100,000. The five countries with the highest ASMR of the LC were Republic of Moldova (ASMR=9.5), Romania (ASMR=7.2), Montenegro (ASMR=6.6), Luxembourg (ASMR=6.3) and Bosnia Herzegovina (ASMR=6.2), respectively. Similarly, lowest ASMR of the LC were in Norway (ASMR=1.7), Belarus (ASMR=1.9). The Netherlands (ASMR=1.9), Iceland (ASMR=2), and Ukraine (ASMR=2.2), respectively. The countries with the highest and lowest ASIR and ASMR in both sexes are observable in Table 1 .
ASIR and ASMR
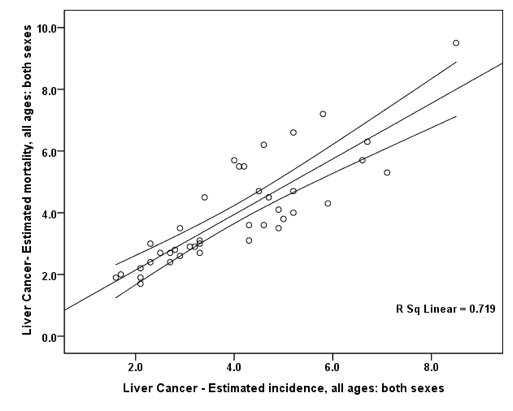
Between the Age-Specific Incidence Rate (ASIR) and Age-Specific Mortality Rate (ASMR) of LC, strong positive significant correlation was observed (r = 0.848; P ≤ 0.001).Also, in males and females, strong positive significant correlation was observed between ASIR and ASMR of LC (r =0.850; p ≤ 0.001) and (r =0.897; P ≤ 0.001), respectively ( Figure 1 ).
ASIR and HDI
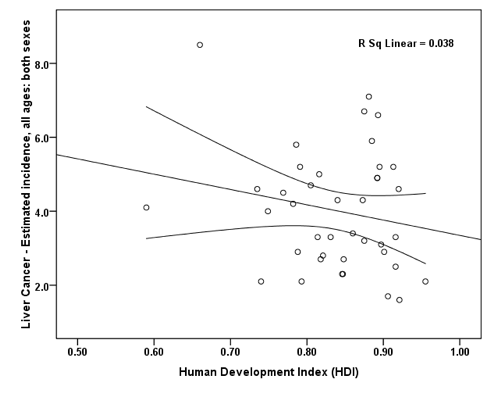
The weak negative correlation was observed between the HDI and ASIR of LC(r=-0.194; P=0.230). Also, ASIR have weak negative correlation with life expectancy at birth (r=-0.064; P=0.695), mean years of schooling (r=-0.290; P=0.070), and GNI (r=0.059; P=0.718) ( Figure 2 ).
In male, a weak negative correlation was observed between the ASIR of LC and HDI (r=-0.114; P=0.482). Also, ASIR have weak positive correlation with life expectancy at birth (r=0.10; P=0.537), weak negative correlation with mean years of schooling (r=-0.235; P=0.144), and weak positive correlation with GNI (r=0.116; P=0.474).
In female, a strong negative correlation was observed between the ASIR of LC and HDI (r=-0.420; P=0.007). Also, ASIR have weak negative correlation with life expectancy at birth (r=-0.164; P=0.312), and GNI (r=-0.187; P=0.248), but has strong negative correlation with mean years of schooling (r=-0.316; P=0.047).
ASMR and HDI
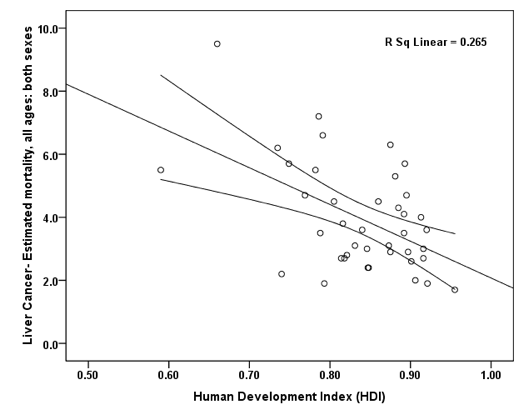
The strong negative significant correlation was observed between the ASMR of LC and HDI (r=-0.515; P =0.001). Also, ASIR have weak negative correlation with life expectancy at birth (r=-0.221; P=0.171), and GNI (r=- 0.236; P=0.143), but has strong negative significant correlation with mean years of schooling (r=-0.421; P=0.007), and ( Figure 3 ).
In male, a strong negative significant correlation was observed between the ASMR of LC and HDI (r=-0.456; P=0.003). Also, ASIR have weak negative correlation with life expectancy at birth (r=-0.196; P=0.225), and GNI ( r=-0.176 ;P=0.276),but has strong negative correlation with mean years of schooling (r=-0.380; P=0.016).
In female, a strong negative significant correlation was observed between the ASIR of LC and HDI (r=-0.613; P≤0.001). Also, ASMR have strong negative significant correlation with life expectancy at birth (r=-0.331, P=0.037), mean years of schooling (r=-0.430; P=0.006), and GNI (r=-0.381; P=0.015).
Discussion
Overall in 2012, European countries have recorded 63,462 cases of LC, Crude Rate was 8.6 and ASIR was 4.3 per 100,000. On the other hand in Europe countries in 2012, 62,191 cases of deaths occurred due to LC, Crude Rate was 8.4 and ASMR was 3.9 per 100,000. Correlation between ASIR and ASMR was 0.848 (P ≤ 0.001), that was statistically significant. In this study between HDI and ASIR of LC a negative correlation was seen about 0.194 (P=0.230), also between HDI and ASMR of LC was a negative correlation about 0.515 (P =0.001).
In European countries, Republic of Moldova (ASIR=8.5), Italy (ASIR=7.1), Luxembourg (ASIR=6.7), France (ASIR=6.6, and Spain (ASIR =5.9), had the maximum ASIR of LC. Four of these countries were in very high level of HDI, but Republic of Moldova was in Medium HDI level. In contrast, five countries with the lowest ASIR of the LC were The Netherlands (ASIR= 1.6), Iceland (ASIR= 1.7), Norway (ASIR=2.1), Belarus (ASIR=2.1), and Ukraine (ASIR=2.1), respectively Ferlay et al., 2015. The HDI in three countries were in very high level of HDI, but in two countries were in high level of HDI Malik, 2013.The results of study that conducted with Chang and et al,. displayed that hepatocellular carcinoma by reason of chronic hepatitis B infection was common in countries with low and medium level of HDI, mostly in Asian and African countries Chang et al., 1997. However, the increased incidence of hepatocellular carcinoma in developed countries was mainly due to increase the prevalence of alcohol use and hepatitis C infection. It seems that the rise of HCC in western countries that have a higher HDI, has been due to hepatitis C infection and alcohol consumption (Liver, 2012). However, ASIR of LC in Europe in 2012 was 6.8 per 100,000 that was less than observed ASIR in the world (ASIR=15.3), Africa (ASIR=12.4), Asia (ASIR =20) and Oceania (ASIR=7.8) Ferlay et al., 2015. In developing parts of the world, especially in Asian countries, cancer is becoming one of the most severe health problems. So that in some of these countries, such as Japan and South Korea, cancer is known as one of the most common causes of deaths. It is expected that if current management strategies and programs do not modified, the number of deaths from cancer by 2020 in these areas will reach 7.1 million cases per year Mackay, 2006.
The distribution of cancers in different parts of the world in terms of human development index is very different, so in regions with very high, high, medium and low HDI, various cancers are classified as the most common cancer. cancer of the lung, breast, colorectal and prostate in areas with very high and high HDI are considered as the most common cancers that almost include half of new cancer cases in this region. Also, in regions with medium and low HDI, in addition to breast, colorectal and lung cancer, cervical cancer, liver and stomach cancer classified as cancers with high incidence and mortality. However, in regions with low HDI, cancers due to infectious agents included a large part of incidence and mortality of cancer Bray et al., 2012Franceschi and Wild, 2013.
The results of this study presented that the ASMR of LC in Europe varies from 1.7 in Norway to 9.5 in Republic of Moldova. The highest ASMR of LC occurred in Republic of Moldova (ASMR=9.5), Romania (ASMR=7.2), Montenegro (ASMR=6.6), Luxembourg (ASMR=6.3) and Bosnia Herzegovina (ASMR=6.2). In these countries only Luxembourg was in very high level of HDI. Similarly, five countries with lowest ASMR of LC were Norway (ASMR=1.7), Belarus (ASMR=1.9), The Netherlands (ASMR=1.9), Iceland (ASMR=2), and Ukraine with (ASMR=2.2) that were in very high and high level of HDI.
This study is an ecological study and its results can be interpreted only at the population level and attribution of the results of this study to individual levels lead to occurrence of ecological fallacy. This study also has some advantages.
The first advantage is that we studied all European countries. So the data have perfect integrity. The second advantage is the novelty of findings because we couldn’t find a study that shows relationship between the ASIR and ASMR of LC with HDI and its components in European countries. Therefore, it is proposed that similar studies in other parts of the word should be done, so that the relationship hypothesis between the incidence and mortality rate of LC and HDI in these regions can be examined.
Conclusion
Correlation between ASIR and ASMR was statistically significant. Also, we were observed a negative correlation between HDI and the ASIR of LC, but between the HDI and ASMR of LC significant correlation was observed. Therefore, increase in the human development index was associated with reduce in incidence and mortality of LC.
Abbreviations
ASIR: Age-specific incidence rate
ASMR: Age-specific mortality rate
HDI: Human Development Index
LC: Liver Cancer
Author contribution
All authors contributed to the design of the research. MS, SIF, SK and HS collected the data. HS, SK and AMH conducted analysis and interpretation of data. All authors drafted the first version. MM, MA, PB, FAB and AMH edited the first draft. All authors reviewed and commented on final draft.
References
-
F.
Bray,
A.
Jemal,
N.
Grey,
J.
Ferlay,
D.
Forman.
Global cancer transitions according to the Human Development Index (2008-2030): a population-based study. The lancet oncology.
2012;
13
:
790-801
.
-
M.-H.
Chang,
C.-J.
Chen,
M.-S.
Lai,
H.-M.
Hsu,
T.-C.
Wu,
M.-S.
Kong,
D.-C.
Liang,
W.-Y.
Shau,
D.-S.
Chen.
Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. New England Journal of Medicine.
1997;
336
:
1855-1859
.
-
J.
Ferlay,
F.
Bray,
P.
Pisani,
D.
Parkin.
Cancer incidence, mortality and prevalence worldwide, version 1.0. IARC CancerBase.
2001
.
-
J.
Ferlay,
H.R.
Shin,
F.
Bray,
D.
Forman,
C.
Mathers,
D.M.
Parkin.
Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. International journal of cancer.
2010;
127
:
2893-2917
.
-
J.
Ferlay,
I.
Soerjomataram,
R.
Dikshit,
S.
Eser,
C.
Mathers,
M.
Rebelo,
D.M.
Parkin,
D.
Forman,
F.
Bray.
Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International journal of cancer.
2015;
136
:
E359-E386
.
-
J.
Ferlay,
I.
Soerjomataram,
M.
Ervik,
R.
Dikshit,
S.
Eser,
C.
Mathers,
M.
Rebelo,
D.
Parkin,
D.
Forman,
F.
Bray.
GLOBOCAN 2012 v1. 0, Cancer incidence and mortality worldwide: IARC CancerBase No. 11. 2013.. International Agency for Research on Cancer Web site Available online: http://globocan iarc fr (accessed on 24 November 2014).
2014
.
-
W.D.
Foulkes,
K.A.
Cooney.
Male Reproductive Cancers. Springer.
2010
.
-
S.
Franceschi,
C.P.
Wild.
Meeting the global demands of epidemiologic transition-The indispensable role of cancer prevention. Molecular oncology.
2013;
7
:
1-13
.
-
M.
Ghoncheh,
A.
Mohammadian-Hafshejani,
H.
Salehiniya.
Incidence and mortality of breast cancer and their relationship to development in Asia. Asian Pac J Cancer Prev.
2015;
16
:
6081-6087
.
-
A.J.
Hall,
C.P.
Wild.
Liver cancer in low and middle income countries. Bmj.
2003;
326
:
994-995
.
-
S.
Hassanipour-Azgomi,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
F.
Towhidi,
S.
Jamehshorani,
H.
Salehiniya.
Incidence and mortality of prostate cancer and their relationship with the Human Development Index worldwide. Prostate International.
2016
.
-
J.
Mackay.
The cancer atlas. Amer Cancer Society.
2006
.
-
K.
Malik.
Human development report 2013. The rise of the south: Human progress in a diverse world. The Rise of the South: Human Progress in a Diverse World (March 15, 2013). UNDP-HDRO Human Development Reports.
2013
.
-
M.
Mohammadian,
A.
Soroush,
A.
Mohammadian-Hafshejani,
F.
Towhidi,
F.
Hadadian,
H.
Salehiniya.
Incidence and Mortality of Liver Cancer and Their Relationship with Development in Asia. Asian Pacific journal of cancer prevention: APJCP.
2015;
17
:
2041-2047
.
-
R.
Pakzad,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
I.
Pakzad,
H.
Salehiniya.
The incidence and mortality of lung cancer and their relationship to development in Asia. Translational lung cancer research.
2015a;
4
:
763
.
-
R.
Pakzad,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
I.
Pakzad,
H.
Salehiniya.
The incidence and mortality of prostate cancer and its relationship with development in Asia. Prostate international.
2015b;
3
:
135-140
.
-
R.
Pakzad,
A.
Mohammadian-Hafshejani,
B.
Khosravi,
S.
Soltani,
I.
Pakzad,
M.
Mohammadian,
H.
Salehiniya,
Z.
Momenimovahed.
The incidence and mortality of esophageal cancer and their relationship to development in Asia. Annals of translational medicine.
2016;
4
.
-
R.
Pakzad,
A.
Mohammadian-Hafshejani,
M.
Mohammadian,
I.
Pakzad,
S.
Safiri,
S.
Khazaei,
H.
Salehiniya.
Incidence and Mortality of Bladder Cancer and their Relationship with Development in Asia. Asian Pac J Cancer Prev.
2015c;
16
:
7365-7374
.
-
H.
Rafiemanesh,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
Z.
Sepehri,
R.
Shamlou,
H.
Salehiniya,
F.
Towhidi,
B.
Makhsosi.
Incidence and Mortality of Colorectal Cancer and Relationships with the Human Development Index across the World. Asian Pacific journal of cancer prevention: APJCP.
2015;
17
:
2465-2473
.
-
K.-R.
Wei,
X.
Yu,
R.-S.
Zheng,
X.-B.
Peng,
S.-W.
Zhang,
M.-F.
Ji,
Z.-H.
Liang,
Z.-X.
Ou,
W.-Q.
Chen.
Incidence and mortality of liver cancer in China, 2010. Chin J cancer.
2014;
33
:
388-394
.
Comments

Downloads
Article Details
Volume & Issue : Vol 4 No 03 (2017)
Page No.: 1185-1197
Published on: 2017-03-20
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
- HTML viewed - 6343 times
- Download PDF downloaded - 1987 times
- View Article downloaded - 14 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}