

Mortality rate associated with hospital acquired infections among burn patients
Copyrights: Saima Aslam Bharwana, Mujahid Farid, Shafaqat Ali, Muhammad Rizwan, Muhammad Nadeem, Muhammad Waqas Haider, Hafiz Muhammad Tauqeer, Rasahm Sallah-Ud-Din, Rehan Ahmad, 2016. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Hospital acquired infections (HAIs) are the major contributors of mortality associated with burn injuries. The aim of this research was to document the antecedents affiliated with major burn injuries, hospitalization and mortality in burn patients. We performed a single center prospective study of patients admitted during 3 months period (April-June 2014) in burn wards of government hospital. There were 100 patients in this investigation which were observed weekly. The inclusion criterion was based on the shifting of patients from emergency to the wards after initial treatment of more than 24 h. Variables included were age and gender of the patient, the percent total body surface area (%TBSA) burn, the cause of the burn. Mean age of patients was 30.29 years. More females (55.67%) were admitted than males (44.32%). The total body surface area (%TBSA) burnt were from 15%- 95% respectively moreover children were more sensitive to hospital acquired infections (HAIs) and mortality rate was 34% in children with mean age of 5 years and disability of body parts were 42% among 75% were females. Whereas the most common (HAIs) were primary blood stream (PBS) with mean value of 30.50, wound infections (WIS) were at second prevalence with mean value of 27.50, followed by sepsis (S) and pneumonia (P) 10.33, eye infections (EIs) 4.833 and urinary tract infections (UTIs) 2.667. Factors significantly (p-value= 0.000) associated with increased duration of hospitalization caught HAIs mortality include the age and gender of the patient, the cause of burn, inhalation injury, the region affected and %TBSA burnt. It concluded that the mortality was very much dependent on age and gender of the patient, burn causes, affected area as well as %TBSA burnt are considerable factors in determining the relationship of HAIs and whether the patients will survive or knuckle to injuries. Better compliance techniques, stricter control over disinfection and sterilization practices and usage of broad spectrum antibiotics, and reduction of the environmental contamination are required to reduce the HAIs rates among burn patients.
Introduction
The main objective of this attempt is to provide valid estimates of the risk of death following by burn injuries which have long and extensive history and yet little have changed during the time. Measures to prevent and/or treat and minimize infections are essential for the survival of patients with extensive burns. Many past studies indicated that infection is correlated to mortality. In patients with less extensive burns, infections may increase morbidity and hospital stay McManus, 1994. To assess the quality of care and to identify risk factors for infection and other complications, a prospective monitoring system is necessary. In this prospective study we describe a series ho HAIs that are possible outcome of burn injuries.
Burn injuries portrayed public health issues among developing as well as developed nations Tarim et al.,2005. Burn injuries and associated mortality framed in history as most prevalent cause of deaths nationwide Neghab et al., 2006. Among annual reported injuries in USA two million are ranked in burn category (US fact sheet 2000). The mortality in South Asia extended over 10/100,000 burn injuries Tredget et al., 1990. In biggest city of Pakistan, Karachi the adult mortality rate due to burns was, 6.8/100,000 for men and 14.1/100,000 for women, respectively in the year of 2002 World Health Organization, 2002. The epidemiology of burns vary significantly around the globe and is very much inveigled by variable factors like, poor workplace health and safety management, lack of training at work, Delgado, 2002 social and cultural set up Batra, 2003 that can create stress and leads to suicidal attempts Lari and Alaghehbandan, 2003.
Burn injuries often affect much more than just the tissue damage, burn wound represents a susceptive site appertain to colonization of endogenous and exogenous organisms. Its obvious outcome is increased risk of mortality affiliated with hospital acquired infections Markley, 1968. Despite effective burn injuries management infection still present significant risk of mortality ranging from 50–75% Luterman et al., 1986Mozingo DW, 1998. Hospital acquired infections are correlated to mortality McManus, 1994. Infection is one and only significant indicator of outcome in the field of quality assurance in burn management Helvig et al., 1995. Sepsis is a leading causes of death among hospitalized patients Angus et al., 2001.
Overcrowding in developing countries increases the risk of HAI. No prospective study of HAI has been reported from Pakistan to the best of our knowledge. Therefore, this study was done in a private hospital with the capacity of 120 burn patients in two burn wards to reveal the occurrence rates of HAI which leads to increased mortality rate, organisms responsible, their antibiotic resistance, factors affecting the outcome, and to monitor the environmental health and safety with patient care perspective. The following (HAI) were considered: primary bloodstream, burn wound infections, pneumonias, sepsis and infections of eyes.
Patients and methods
Burn Units
From the overcrowded emergency of hospital burn patients were shifted to the burn units each with capacity of sixty beds. This was a case series studies designed over 90 days period (March- May 2014) with detailed weekly investigations. This study was conducted in a semi-governmental hospital of biggest industrial city (Faisalabad) of Punjab Pakistan. The hospital is single large health care facility for burn patients. There is no private or governmental facility designated for burn patients however the city is well known for industry and so workplace fire hazards occurred frequently in the area. The burn patients have the only hope of this blessing otherwise they have been referred to far away locations which is sometimes life threatening and can cause deaths on the way to other burn hospitals. The study included all burn injury patients who primarily administered to and were managed at burn units. Those patients who presented more than 24 h after injury and shifted from emergency to the burn wards were included in this study while those who were initially managed at some other hospital were excluded from the study. The patients who referred to the other hospitals before shifting to the burn ward were also an exclusion. Patients with minor burns were discharged after emergency management with requisite medication and follow-up advice. Informed ratification was taken from the burn patients and hospital ethic committee for victim inclusion in the study. This study is not to criticize or critically target a person and/or organization for being responsible but to create awareness among the target group.
Initial Assessment
Initial assessment were made by through preliminary survey of burn wards and following necessary investigations were recorded like total body surface area (TBSA), Causes of burn, age, gender and type of prevalent hospital acquired infections (HAIs). The demographic profile of the burn patients were recorded in accordance with social factors like place endured burn injury, TBSA burnt, depth burnt and outcome in terms of survival or mortality. As per the protocol of burn ward, all burn victims were initially managed according to life saving standard. Moreover some factors contributed to HAIs among burn patients and increased the mortality. A non-medicated soap was used to wash hands and health compliance was poor. In general condition patient’s wounds were washed at washing area of ward before dressing to remove exudates and then were transported via ward trolleys and/or wheel chairs which are usually not disinfected between two patients. However some children were washed on their beds and usually bed sheets were not changed on daily basis. Most of the patients were catheterised to monitor urine output for fluid management. Wound cleaning, topical antibiotics, and specific dressing were frequently applied after assessment by surgeons. Maintenance of central venous line, plasma and blood transfusion, ventilation, oxygen supply, nebulization, temperature monitoring and other shared practices were common. The caretaker of patients were advised to keep necessary things by themselves to avoid infections like thermometer, nebulization mask, disinfectant, gloves etc.
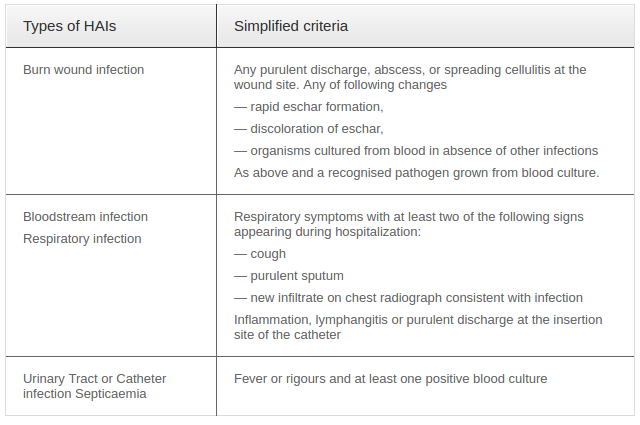
Data Collection
97 patients with 15–95% of total body surface area burned were included in this study conducted for 90 days inspection from March to May 2014. The patients were examined on weekly basis and followed from discharge to death. The major contributing factors of HAIs and associated mortality rate were observed closely. The personal profile of patients were observed with burn details whereas wound conditions, infections proliferation, antibiotic provision and all other required procedures and treatments adopted for life saving were noted thoroughly. Criterion for hospital-acquired infections was followed as per described by WHO/CSR 2002 and presented in Table 1 . Environmental sampling was done twice a month for the specified period of ninety days. The environmental sampling was based on close observations and qualitative inquiry of hygiene practices for use of dressing and bandage, dressing trolley, disinfectants, tables, bed sheets, thermometer, nebulizer machine and mask, normal saline, tabs, washrooms, kitchen, mattresses, refrigerator, medicine trolley, cotton rolls/swaps, lookers, Heating and ventilation systems, electric switches, washing area, wheel chairs, benches, equipment, pillow, towels, blankets, stands, separation curtains and medicines supplied regularly (creams, tablets, injections and other). This collected data was recorded on a simple self-structured questionnaire checklist for the hygiene practices.
Statistical Analysis
Minitab 17 version was used for analysis of variance and one way ANOVA was performed for the collected data in order to analyze the differences between group means and their associated procedures. Descriptive statistics for distribution, mean age and dispersion were calculated. To determine whether there exists a significant relationship between variables assessed and the hospital acquired infection and outcome (mortality) ANOVA was used All values were considered significant when below 0.05 (p < 0.05).
Results
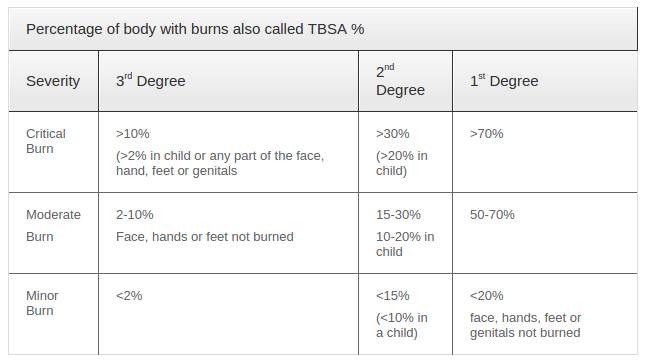
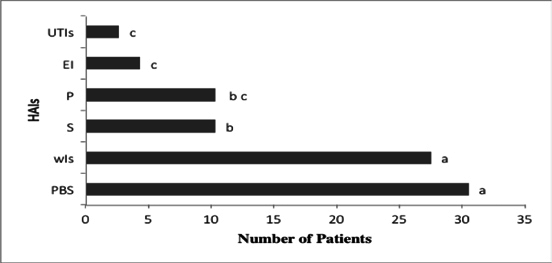
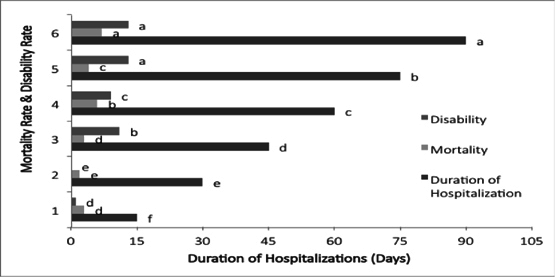
During the 90 days period of study 97 burn patients met the inclusion criterion to evaluate the mortality rate due to hospital acquired infections which were prevalent among victims and cause of deaths. The simplified criteria of hospital acquired infections were followed according to the world health organization and (CDS 2002) and is presented in the Table 1 . This criteria helped to recognize the HAIs on qualitative basis and presented a clear picture of burn infections.Hospital-acquired infections were defined based upon CDS case definitions presented in Table 1 . The Table 2 depicted the severity of burn which is recommend for the calculation of TBSA%. This is totally dependent on age and area of burn therefore children and some specific areas like genitals, face, feet and hands etc. can contribute to make the causality worse. There were 12 children in the age of 0-12 (9 females, 3 males) in the burn wards (exclusion of pediatric ward of children) and out of these 12 the mortality rate was 42% and disability was 33% and most of the causalties were below 10 years of age. These were followed for 90 days period and if trend prevails it can be worse. The Table 3 showing the distribution and role of age and gender among burn patients and out of total 97 patients (54 females and 37 males) i.e. 55.67% females and 44.32% males both with the mean adult age of 30.29 years and greater were the number of person from 21-40 years of age and the general cause of burn among these patients were fire, electrical and/ or chemicals which generally exist at home or industry. Greater number of females in this age group was victim either because of negligence at home work activities like (cooking, washing) or may be due to social pressure (suicidal cases) there were quite few females who got burn because of any health issues like (heart attack, epilepsy). Whereas the more male were injured due to industrial accidents i.e. (fire, boiler steam). So the table 4 showing the types and places of burn according to it 43.29% burn cases were registered as fire burns or may be categorized as thermal burns and the main cause of these type of burns was home and workplace exposures to fire hazards. There were (37.11%) electrical cases which were prevalent together at home and workplace and also some events were associated with market place. Scalds were common among the children of 1-5 years age and even in toddlers who had contacted with boiled water, milk or sometimes from geysers water by opening hot-water tabs. The percentage of scalds was 13.40%. The least common but the most adverse was chemical burns associated with industrial workers and use of chemicals at workplace and it was 6.18%. The one way ANOVA results for hospital acquired infections (HAIs) are shown in table 5 the p values (p-value = 0.000) for HAIs indicated that the infections were significant at 5% level of significance. The results for ANOVA test lead to the decision that HAIs are significant cause of mortality in burn patients. There was also some controlled and uncontrolled factors in the above analysis which resulted in variability of infection prevalence. The Figure 1 showing results of mean values along with letter grouping (Tukey’s Test). The result indicated that HAIs prevalent in burn wards and are significant cause of mortality and among these infections the more prevalent are primary bloodstream infections (PBS) and burn wound infections (WIs) with the mean values of 30.5 and 27.5 respectively. Whereas sepsis (S) and pneumonia (P) having 10.33 mean value and are 3rd largest infection factor for increased mortality rates. The eye infection (EI) were common not only in burn patients but some caregivers were also suffering in it the mean value was 4.33 but these infections were not directly related to deaths in patients. Moreover the urinary tube infections (UTI) related to use of catheter was source of infection among the burn patients who were using for prolonged period. In the specified period of 90 days UTI related deaths were less common but I can be source of death if prolonged use. The qualitative environmental assessment ( Figure 2 ) was done twice a month and 34 sampling points were observed from where 68 inspected elements give were collected in first month out of which 17 were correct and 51 were not correct or unhygienic. In second month total 60 samples were inspected qualitatively for effective hygiene practice out of which 38 were in good condition but 22 were posing threat of spreading toxicity among burn patients. In the 3rd month again quarterly 71 elements were inspected out of which 30 were significant risk to the health of patients and caregivers. The mortality rate among burn patients were evaluated on the basis of HAIs prevalence which is shown in the Figure 3 mortality and disability increased with the passage of time in hospital andwas increased from 3 deaths to 7 deaths during the period of study and altogether there were 25 deaths among 97 cases. Whereas disability was also significant and it was increased from 1 to 13 patients during 90 days among 97 patients.

Discussion
To the best of our knowledge this study is first of its type which focused to evaluate the mortality rates associated with HAIs among burn patients which is measured during 90 days period and dependent on the number of patients admitted during that time period. This is a short retrospective study a long series study was done by Iqbal et al., 2013 and analysis of 716 cases was done for preventable burn injury issues Siddiqui, 1998. Some locally published research papers based on short studies mainly targeted epidemiology of adult burn patients only Marsh et al., 1996Muqim et al., 2008. The presentation of burn injury and its management was also done Khan and Khattak, 2006. Patients with 15–95% TBSA were enrolled because those with <15% are usually discharged within a day and followed up for visits only while ones with 95% survived for a week due to other factors like age etc. Since we also excluded patients transferred from other hospitals, infections not existing at the time of admission, but developing during hospital stay were considered hospitalacquired infections. The HAIs prevalence was an important and significant predictor of outcome among burn causalties also described by Taneja et al., 2004. HAIs caused mortality and morbidity among the patients in 90 days and there were total 25 deaths constituting 27.77% mortality and there were 47 cases of disability constituting 48.45% due to infection and burn which is comparable to other studies Appelgren et al., 2002 and Wurtz et al., 1995 who evaluated nosocomial infection which were capable to become worse with the passage of time and prolonged stay in hospital Wong and Ngim, 1995 which is also considered by Khaliq et al., 2013 focusing on factors associated with duration of stay and mortality among burn patients in Karachi, Pakistan. The primary bloodstream infections and wound infections were more common and significant cause of deaths also observed in other studies like Taneja et al., 2004. Sepsis and pneumonia were second culprit of HAIs and leads to death in developing countries also reported Tanriover et al., (2006) in contrast a study showed, sepsis is a significant cause of increased rate of mortality in developed countries Angus et al., 2001De Coppi et al., 2007Frikha et al.,2005 in contrast to this Degoricija et al., (2006) reported sepsis can be treated with intensive medical care and antibiotics use. Whereas pneumonia which may be ventilator associated or ICU associated contributed equally to promote HAIs as it is found in other related studies Chastre and Fagon, 2002Rello et al., 2002. Most of the patients were catheterised but UTI incidence were significantly lower this may be due to early removal of catheter.
Moreover in our findings, female patients were more (A, 1999) than males and predominant involvement of males is reported by other published studies Kobayashi et al., 2005Tarim et al., 2005. In our observation that more adults constituted the magnitude of the burn patients which is integrated in several studies Hemeda et al., 2003Marsh et al., 1996OM, 2004Taneja et al., 2004.
This investigation resulted that fire burns were the predominant burns among the hospitalised cases which is corresponding to various researchers’ findings Calder, 2002Iqbal et al., 2013Maghsoudi and Samnia,2005. Whereas scalds were common among children burnt by boiled water or milk or any liquid stored in greater quantities in easy access of children however scalds have been reported as the most common burns among children by most of the studies Calder, 2002Iqbal et al., 2013Komolafe et al., 2003Saadat, 2005Siddiqui, 1998.
The home considered to be a significant burn injury contributor for females (housewives and maids) reported by Tarim et al., 2005 also evident that home environment constitute large number of risk factors attached to fire burns. In this study there was significant number of females and children burned at home due to multitude of hazards existed Iqbal et al., 2013There was another activity which contributed in homework fires and that was the use of mosquito repellants and or gas heaters in the night and left them unattended. The reported scald injuries were also related to home and most common among them was burnt by hot liquids (water, milk, tea) toddlers and the kids of age group 1-5 were the victims of these burn injuries and caused deaths similarly its socioeconomic and cultural influence in children were studied by Daisy et al., (2001). Risk factors for burns in children: crowding, poverty, and poor maternal education were described in the study of Delagado et al., (2001). Whereas electrical burn injuries were also associated with home, industry and market as short circuiting can occur anywhere but children involved while contact with high voltage wires during playing on roofs or during kite flying with iron wires. Similarly poor maintenance of electrical appliances and transformers near the roofs of houses are also significant contributor of electrical incidents. There was significant factor of disability due to electrical burn injuries. Some females were victim of suicidal attempts due to social pressure or family reasons also reported Alaghehbandan et al., 2010Maghsoudi and Samnia,2005Tsati et al., 2005 whereas some female causalities occurred due to diseases like heart attack and/or epilepsy attack while cooking reported as medical reasons by Saadat, 2005Siddiqui, 1998Tsati et al.,2005.
Industries also playing considerable role in increasing the extent of burn hazards like there were some cases related to young male workers who were victimized while on working with boiler and its bursting put them to death. There was another industry related case which was deliberate contact with explosive chemicals stored and kept in unlabelled storage boxes and new untrained workers contacted without knowing these death tolls. We did not find any significant difference in the frequency of burn injuries over the study period it is in accordance with a long study conducted by Iqbal et al., 2013.
Similarly crowding in wards increased the people's burden than capacity and leads to increased environmental contamination cases which in turn sheds its burden on proliferation of infections not only among patients but also among caregivers. The other significant reason for toxicity was burn wound which can easily be affected by xenobiotic therefore poor sterilisation and disinfection practices, lack of hygienic conditions and isolation facilities which are important in reducing risks associated with HAIs reported by McManus et al., 1994, inadequate hand washing and lack of awareness were some of the reasons for higher wound infection and sepsis among burn patients also reported by Shirani et al., 1988.
The mortality rate in our study was 25.77% while Tariq et al., (2013) reported 14% for the hospitalised subset of patients, whereas Khaliq et al., 2013 reported 24.69% and 26.38% respectively for males and females. Haik et al. (2003) reported an overall mortality rate of 4.4% among burn patients. Similarly 27% mortality was observed by Laloe, (2002) and Yang et al., (2008) reported 9.08% in the paediatric population.
Conclusion
Hospital acquired infections and associated mortality of burn patients is dependent upon the age and gender of the patient; cause of burn, %TBSA burnt and parts of body affected and also the length of hospitalization. Greater the proliferation of HAIs the greater is the mortality associated with it among burn patients. The significant increase in female mortality strongly necessitates the urge of creating awareness among public and educate them regarding safe workplace environment not only at home but also at work. Elimination of hazards and proper maintenance of electrical appliance frequently in contact with females for safer home environment. Furthermore, installation of fire extinguishers, smoke detection alarms, sand buckets and proper ventilation can also be helpful to lower the risks associated together with home and industry. Domestic violence must be managed to reduce suicidal attempts among female burn cases. Home safety should be ensured particularly with reference to children and women. Parents should not leave hazardous elements unattended and in reach of children community awareness and education of mothers can be a significant effort to reduce burn cases of scalds and fire. Government and all the relevant authorities play their part in collaboration to manage this challenging issue. Our studies provided a short term evaluation related to HAIs and associated mortality rate and found females and children are at high risk due to unsafe home environment and youth is victimized due to unsafe industrial practices. These should be targeted in management program on priority basis. Whereas there is dire need of regional burn centers with increased capacity and covering all the cities. Some deaths were because of unavailability of ventilator so ventilators must be increased specially in burn units. At the end we suggest some more detailed and prolonged study focusing multitude of burn injury issues to improve our results.
References
-
WHO
World Health Organization.
In SpringerReference (Springer Science + Business Media).
.
-
L.
A.
Clinical audit and probit analysis of mortality data of burned patients admitted at PGIMER over a period of one year. Dissertation submitted in partial fulfillment of the requirement for the degree of M.ch (Plastic surgery) of PGIMER December. 1999
.
-
R.
Alaghehbandan,
A.R.
Lari,
M.-T.
Joghataei,
A.
Islami.
The Role of Marital Status, Literacy, and Urbanity in Suicidal Behavior by Burns in the Province of Khorasan, Iran. Community Ment Health J.
2010;
47
:
181-185
.
-
D.C.
Angus,
W.T.
Linde-Zwirble,
J.
Lidicker,
G.
Clermont,
J.
Carcillo,
M.R.
Pinsky.
Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Critical Care Medicine.
2001;
29
:
1303-1310
.
-
P.
Appelgren,
V.
Björnhagen,
K.
Bragderyd,
C.E.
Jonsson,
U.
Ransjö.
A prospective study of infections in burn patients. Burns.
2002;
28
:
39-46
.
-
A.K.
Batra.
Burn mortality: recent trends and sociocultural determinants in rural India. Burns.
2003;
29
:
270-275
.
-
F.
Calder.
Four years of burn injuries in a Red Cross hospital in Afghanistan. Burns.
2002;
28
:
563-568
.
-
J.
Chastre,
J.-Y.
Fagon.
Ventilator-associated Pneumonia. Am J Respir Crit Care Med.
2002;
165
:
867-903
.
-
P.
De Coppi,
G.
Bartsch,
M.M.
Siddiqui,
T.
Xu,
C.C.
Santos,
L.
Perin,
G.
Mostoslavsky,
A.C.
Serre,
E.Y.
Snyder,
J.J.
Yoo.
Isolation of amniotic stem cell lines with potential for therapy. Nature.
2007;
biotechnology25
:
100-106
.
-
J.
Delgado.
Risk factors for burns in children: crowding, poverty, and poor maternal education. Injury Prevention.
2002;
8
:
38-41
.
-
N.
Frikha,
M.
Mebazaa,
L.
Mnif,
N.
El Euch,
M.
Abassi,
A.M.
Ben.
Septic shock in a Tunisian intensive care unit: mortality and predictive factors. 100 cases.. La Tunisie medicale.
2005;
83
:
320-325
.
-
E.I.
Helvig,
J.
Upright,
B.J.
Bartleson,
R.J.
Kagan.
Development of Burn Outcomes and Quality Indicators. Journal of Burn Care & Rehabilitation.
1995;
16
:
208-211
.
-
M.
Hemeda,
A.
Maher,
A.
Mabrouk.
Epidemiology of burns admitted to Ain Shams University Burns Unit, Cairo, Egypt. Burns.
2003;
29
:
353-358
.
-
T.
Iqbal,
M.
Saaiq,
Z.
Ali.
Epidemiology and outcome of burns: Early experience at the country’s first national burns Centre. Burns.
2013;
39
:
358-362
.
-
M.F.
Khaliq,
M.M.
Noorani,
U.A.
Siddiqui,
E.
Al Ibran,
M.H.
Rao.
Factors associated with duration of hospitalization and outcome in burns patients: A cross sectional study from Government Tertiary Care Hospital in Karachi, Pakistan. Burns.
2013;
39
:
150-154
.
-
H.
Khan,
A.M.
Khattak.
A study of prevalence of malaria in adult population of DI Khan, Pakistan. iomedica.
2006;
22
:
99-104
.
-
K.
Kobayashi,
H.
Ikeda,
R.
Higuchi,
M.
Nozaki,
Y.
Yamamoto,
M.
Urabe,
S.
Shimazaki,
A.
Sugamata,
N.
Aikawa,
N.
Ninomiya.
Epidemiological and outcome characteristics of major burns in Tokyo. urns.
2005;
31
:
S3-S11
.
-
O.O.
Komolafe,
J.
James,
L.
Kalongolera,
M.
Makoka.
Bacteriology of burns at the Queen Elizabeth Central Hospital, Blantyre, Malawi. Burns.
2003;
29
:
235-238
.
-
A.R.
Lari,
R.
Alaghehbandan.
Epidemiological Study of Self-Inflicted Burns in Tehran, Iran. Journal of Burn Care & Rehabilitation.
2003;
24
:
15-20
.
-
A.
Luterman,
C.C.
Dacso,
P.W.
Curreri.
Infections in burn patients. The American Journal of Medicine.
1986;
81
:
45-52
.
-
H.
Maghsoudi,
N.
Samnia.
Etiology and outcome of pediatric burns in Tabriz, Iran. Burns.
2005;
31
:
721-725
.
-
K.
Markley.
The role of bateria in burn mortality. Ann NY Acad Sci.
1968;
150
:
922-930
.
-
D.
Marsh,
A.
Sheikh,
A.
Khalil,
S.
Kamil,
Z.
Jaffer uz,
I.
Qureshi,
Y.
Siraj,
S.
Luby,
S.
Effendi.
Epidemiology of adults hospitalized with burns in Karachi, Pakistan. Burns.
1996;
22
:
225-229
.
-
A.T.
McManus.
A Decade of Reduced Gram-negative Infections and Mortality Associated With Improved Isolation of Burned Patients. Arch Surg.
1994;
129
:
1306
.
-
M.A.
Mozingo DW,
BA
Pruitt Jr.
Infections of burn wounds. In: Bennett JV, Brachman PS, editors. Hospital infections. Philadelphia. Lippincott-Raven Publishers.
1998;
:
587-59
.
-
R.-u.
Muqim,
Q.-E.A.
Jan,
M.
Zarin,
M.T.
Khan,
J.
Iqbal,
I.M.
Khan,
M.
Aurangz,
A.
Wazir.
Laparoscopic Repair of Ventral Hernia an Early Experience at Khyber Teaching Hospital Peshawar. World Journal of Laparoscopic Surgery with DVD.
2008;
:
35-38
.
-
M.
Neghab,
A.
Rajaei Fard,
M.
Habibi,
A.
Choobineh.
Home accidents in rural and urban areas of Shiraz 2000-02. 2006
.
-
O.
OM.
Burns in Africa. Afr J Trauma.
2004;
2
:
20-2
.
-
J.
Rello,
D.A.
Ollendorf,
G.
Oster,
M.
Vera-Llonch,
L.
Bellm,
R.
Redman,
M.H.
Kollef.
Epidemiology and Outcomes of Ventilator-Associated Pneumonia in a Large US Database. Chest.
2002;
122
:
2115-2121
.
-
M.
Saadat.
Epidemiology and mortality of hospitalized burn patients in Kohkiluye va Boyerahmad province (Iran): 2002-2004. Burns.
2005;
31
:
306-309
.
-
K.Z.
Shirani,
A.T.
McManus,
G.M.
Vaughn,
W.F.
McManus,
B.A.
Pruitt,
A.D.
Mason.
Effects of Environment on Infection in Burn Patients. Journal of Burn Care & Rehabilitation.
1988;
9
:
678
.
-
N.
Siddiqui.
Burn-injury is preventable: An analysis of 716 cases in a burns unit. Journal of the College of Physicians & Surgeons Pakistan.
1998;
8
:
148-152
.
-
N.
Taneja,
R.
Emmanuel,
P.S.
Chari,
M.
Sharma.
A prospective study of hospital-acquired infections in burn patients at a tertiary care referral centre in North India. Burns.
2004;
30
:
665-669
.
-
A.
Tarim,
T.Z.
Nursal,
S.
Yildirim,
T.
Noyan,
G.k.
Moray,
M.
Haberal.
Epidemiology of Pediatric Burn Injuries in Southern Turkey. Journal of Burn Care & Rehabilitation.
2005;
26
:
327-330
.
-
E.E.
Tredget,
H.A.
Shankowsky,
T.V.
Taerum,
G.L.
Moysa,
J.D.M.
Alton.
The Role of Inhalation Injury in Burn Trauma A Canadian Experience. Annals of Surgery.
1990;
212
:
720-727
.
-
E.
Tsati,
T.
Iconomou,
D.
Tzivaridou,
E.
Keramidas,
S.
Papadopoulos,
D.
Tsoutsos.
Self-Inflicted Burns in Athens, Greece: A Six-Year Retrospective Study. Journal of Burn Care & Rehabilitation.
2005;
26
:
75-78
.
-
M.K.
Wong,
R.C.K.
Ngim.
Burns mortality and hospitalization time — a prospective statistical study of 352 patients in an Asian National Burn Centre. Burns.
1995;
21
:
39-46
.
-
R.
Wurtz,
M.
Karajovic,
E.
Dacumos,
B.
Jovanovic,
M.
Hanumadass.
Nosocomial infections in a burn intensive care unit. Burns.
1995;
21
:
181-184
.
Comments

Downloads
Article Details
Volume & Issue : Vol 3 No 09 (2016)
Page No.: 3(9):790-799
Published on: 2016-09-29
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
- HTML viewed - 8328 times
- Download PDF downloaded - 2223 times
- View Article downloaded - 9 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}