

Copyrights: Vali Sarsangi, Hamid Salehiniya, Mitra Hannani, Milad Ahmadi Marzaleh, Yaser Salim Abadi, Fatemeh Honarjoo, Alireza Sanei Dehkordi, Milad Derakhshanjazari, 2017. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: Nurses often experience occupational accidents and injuries. The mental workload is one of the factors that often cause tiredness. Perilous behaviors possibly occur more in tired persons resulting in injuries. The aim of the study was to evaluate the correlation between mental workload and nursing occupational accidents in public hospitals of Kashan, as well as factors affecting them.
Methods: The analytic-descriptive study described herein consisted of nursing staff from public hospitals of Kashan, Iran. Information was collected using a three-part questionnaire from a selected clustery of 406 nursing personnel in 2016. The questionnaire was used to collect demographics, assess mental workload (per the National Aeronautics and Space Administration Task Load Index (NASA-TLX)), and assess frequency of accidents. The data were analyzed using SPSS software version 16.
Results: A total of 455 occupational accidents were recorded for 2016 with about 2.27±1.21 accidents per nurse. The minimum and maximum scores for frustration and effort were 47.82 ± 30.91 and 78.61 ± 18.15, respectively. The mental workload mean was calculated as 69.49 ± 15.69. In total, 120 (32%) nurses experienced occupational accidents. There was a significant positive correlation between mental workload, mental need and physical need with occupational accidents (P<0.05).
Conclusion: Occupational accidents are affected by mental workload. Taking actions to decline mental workload may result in a decrease of occupational accidents.
Introduction
The Texas Therapeutic Institute has classified hospitals as one of five occupational dangerous settings in terms of injuries and occupational diseases Owens, 2007. Overall, there are numerous biologic dangers, such as from contact with infectious factors (e.g. transmitted by blood or air), and from contact with chemical materials (e.g. anesthesiology and sterilizing gases, antiseptics, etc.). Additionally, there are physical dangers (e.g. from contact with ionizing rays), immune and ergonomic factors (which can lead to musculoskeletal injuries and disorders), as well as socio-psychotic and organizational factors (such as mental and shift stresses). All the aforementioned can threaten health of personnel in health care centers Alavi, 2014Levy, 2006. In health care systems, the nursing cadre is under greater danger than other groups due to high demands of patient care and administration of treatments (sometimes biologically risky) to patients.
In Iran, 80% of occupants of the health care system are nurses. According to the National Association of Professional Safety in the United States of America, nursing is among the top 40 professions in which staff develop diseases related to work-related pressure Safari et al., 2013. Nursing is a stressful job with a high rate of occupational accidents and injuries Alavi, 2014.
According to a report by the Bureau of Labor Statistics, a high rate of occupational accidents was allocated to nursing in the United States; approximately 8.7 occupational accidents occur annually for every 100 permanent nurses. In fact, nursing profession ranks 7th among professions to have the greatest loss of working days due to accidents Gershon et al., 2007. Some studies have been conducted in Iran which are related to safety and health of nurses (including nursing students). These studies have reported that the frequency of needle stick injury, contact with blood, and contact with bodily fluids are approximately 31.1%, 41.7%, and 84.8%, respectively, each year Aghajanlou et al., 2007. Moreover, other studies have reported that the work environment for nurses can be dangerous, and that nurses are at significant risk for on-the-job accidents and injuries.
One of the vital factors affecting behavior and performance of nurses is mental workload Kohn et al., 2002. Mental workload is the mental effort or concentration required during tasks Kohn et al., 2002. It has also been defined as the mental/cognitive need or analytic effort to deal with the needs of workers/ staff and performance under time-driven, physical and environmental demands Neill, 2011. If the mental workload is more than the normal workload, individual performance deficit will emerge Ozkan et al., 2015. High workload and long hours of overtime are the two key factors leading to tiredness Young et al., 2008. Studies indicate that occupations with high workload can cause impaired memory, damage to thinking processes, irritability, and decreased learning due to tiredness and inappropriate working schedules Mohammadi et al., 2013. Ozkan et al. (2014) showed that there is a significant positive correlation between mental workload and the signs of embarrassment and interpersonal sensitivities Ozkan et al., 2015. Di Stasi (2008) reported that increase of mental workload caused attitudes and beliefs to the mental workload of nursing staff is one of the most important indices for safety assessment in special wards Di Stasi et al., 2009. The main cause of more than 90% of occupational hazards (and 70% to 90% of work-related accidents) is human error Ghasemi et al., 2011. When the mental workload is more tolerable than one’s tolerance ability, the thinking process will be affected. Thus, the possibility of taking perilous behaviors will increase, as will the exposure and frequency of accidents.
Findings of previous studies have shown that mental workload and occupational accidents are high among nurses. Therefore, this study aims to evaluate the correlation between mental workload and occupational accidents among nurses of public hospitals in Kashan, Iran. As well, this study seeks to understand the factors and variables (e.g. demographics) which may affect mental workload (as categorized by the National Aeronautics and Space Administration Task Load Index (NASA-TLX)).
Materials - Methods
This analytic-descriptive study was conducted in Kashan, Iran in 2016. The study population consisted of nursing staff from all public hospitals in Kashan with at least one year of experience. The following formula was used to determine the sample volume:, in which Z is confidence coefficient (equal to 95% confidence), is standard deviation (estimated as 20.54 in pilot studies performed), and d is measurement accuracy (equal to 2 units). The required sample size was estimated as 406. A three-part questionnaire was used to collect data. The first part of the questionnaire related to demographic information, consisting of gender (male/female), age (year), marital status (single/married), experience (year), occupational status (official, contractual, formal, and staffing plan), and servicing department (general nursing, anesthesia, surgery, or services (e.g. nurses’ aides or aides’ assistants)).
The second part of the questionnaire assessed the mental work load status using the assessment scale of the NASA-TLX, one of the most commonly used tools to evaluate mental workload in terms of individual perspective Cao et al., 2009Holden et al., 2010Holden et al., 2011Safari et al., 2013. Several reports have confirmed the reliability and validity of NASA-TLX to evaluate mental workload Hoonakker et al., 2011Rubio et al., 2004; for instance, Hoonakker et al. (2011) reported the appropriateness of convergent and discriminant validities of the NASA mental workload scale Hoonakker et al., 2011. Mohammadi et al. (2013) approved the validity of the Persian version of the questionnaire, and its internal consistency reliability (Cronbach’s alpha) of 0.847 was estimated to be suitable Mohammadi et al., 2013.
NASA-TLX evaluates the six sub-scales of mental demands, physical demands, time demands, performance, effort, and frustration using a visual scale divided into 0 to 100 as 5-unit sections. Thus, the minimum and maximum scores of each sub-scale are 0 and 100, respectively. The definition and concept of each sub-scale was presented in the questionnaire; the respondents reviewed the definitions to determine the appropriate sub-scale to mark. The mean of the sub-scales represents the mental workload amount and ranges from 0 to 100. A mean <50 is considered acceptable and >50 is considered high. The third part of the questionnaire (two questions) primarily evaluates whether occupational accidents have occurred during the last year and secondly, the number of occupational accidents that have occurred Huang et al., 2006McCaughey et al., 2013Vinodkumar and Bhasi, 2009.
The questionnaire were distributed amongst the participants; questions regarding the questionnaire were explained by the study researchers. The distribution of sub-scale scores were generated and reported as mean ± standard deviation (SD), and minimum (min) and maximum (max) values. Finally, the data obtained were analyzed by SPSS software version 16 via independent t-test, one-tailed variance analysis, chi-square, and Pearson’s correlation coefficient. P values < 0.05 were considered to be statistically significant.
Results
Of the 406 questionnaires distributed, 375 questionnaires were returned (response rate was estimated as 92.36%). The mean age of participants was 32.23 ± 7.26 years. Additionally, the mean experience was calculated as 9.04 ± 6.45 years. One hundred and thirty-nine (37.1%) and 236 (62.9%) participants were male and female, respectively. Two-hundred and seventy-eight were nurses, 33 were surgical technicians, 15 were anesthesiology technicians, and 40 were nurses’ aides or aides’ assistants. Three-hundred and twenty-six participants had irregular shifts compared to 49 with regular shifts. In terms of occupational status, 110 (29.3%) nurses were official, 77 (20.5%) were contractual, 107 (28.5%) were formal, and 81 (21.6%) were part of staffing plan. The mean overtime period was 42.27 ± 20.09 hours.
Table 1 shows the descriptive statistics relating to the mental workload and its subscales, together with occupational accident experience and mean score of accidents. According to Table 1 , the minimum and maximum scores for frustration and effort were 47.82±30.91 and 78.61±18.15, respectively. The mental workload mean was calculated to be 69.49±15.69. In total, 120 (32%) nurses confirmed they had experienced occupational accidents, while 255 (68%) did not experience any occupational accident. Altogether, 455 occupational accidents occurred over the previous year; the average number of accidents per nurse was 2.27 accidents (range of 0 to 11).
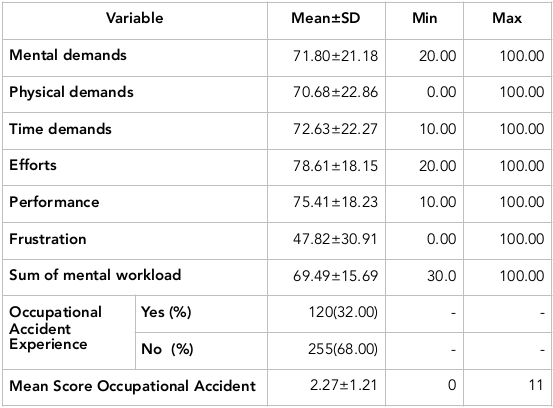
Table 2 depicts the correlation between mental workload and individual characteristics (i.e. demographic variables). According to Table 2 , there was an insignificant difference between mental workload in men versus women (p=0.128). However, there was a significant difference in mental workload among the various age groups (p=0.049); the greatest significant difference was observed in higher aged groups. There was an insignificant difference between mental workload and experience (p=0.204) or hours of time in the week (p=0.735). The mean of mental workload in personnel with regular shifts (70.25 ± 15.66) was significantly higher than in personnel with irregular shifts (64.40 ± 15.05) (p=0.015). A higher mental workload was observed for anesthesiology technicians (73.33 ± 12.50), but no significant difference was observed for the other occupational groups (p=0.288).
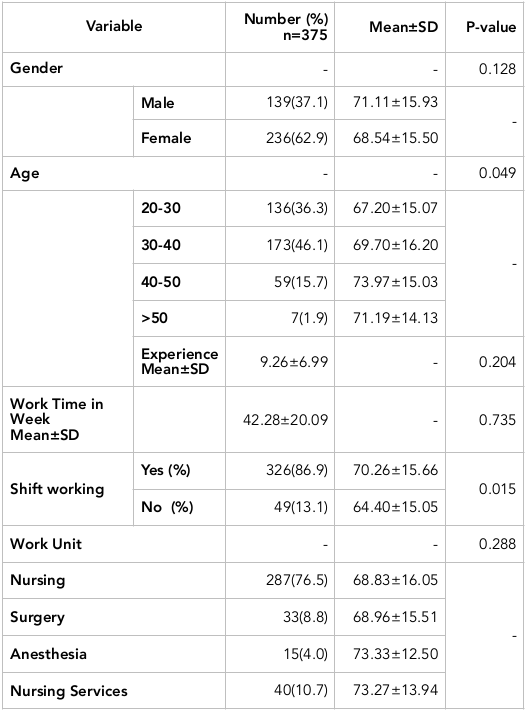
Table 3 indicates the correlation between individual characteristics (i.e. demographic variables) with occupational accident experience and mean of accidents. According to Table 3 , there was a significant difference in occupational accident experience in men versus women (p=0.012). The mean of accidents for men (1.30) was significantly higher than for women (1.16) (p=0.032). Moreover, a significant difference was observed in occupational accident experience (p=0.049) and occupational accident number (p=0.043) for the different occupational groups. There was an insignificant (p>0.05) correlation of accident experience to nursing years (experience), or to hours of time per week. Also, there was no significant correlation between occupational accident and shift (p>0.05), and no correlation to work unit (p=0.081). However, there was a significant difference in the mean of occupational accidents in the different wards (p=0.034).
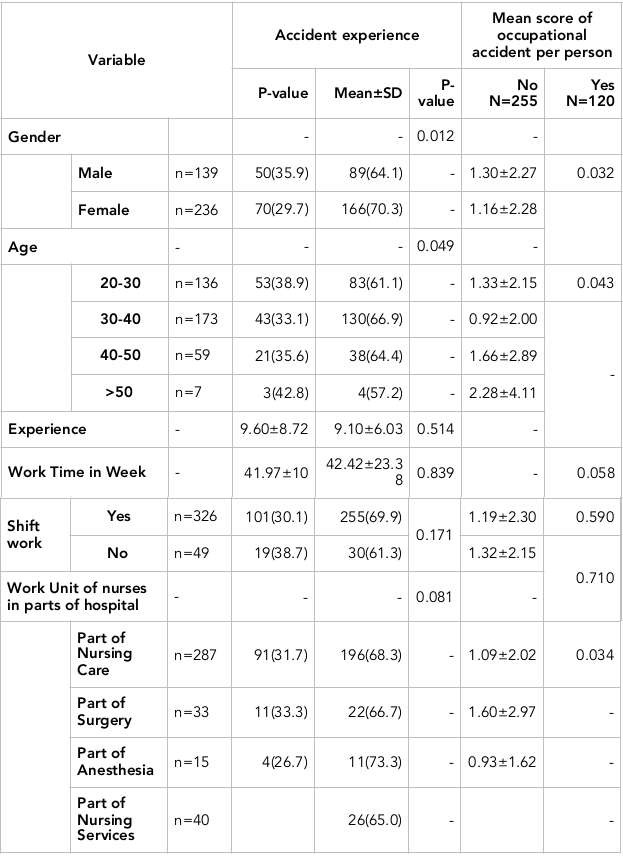
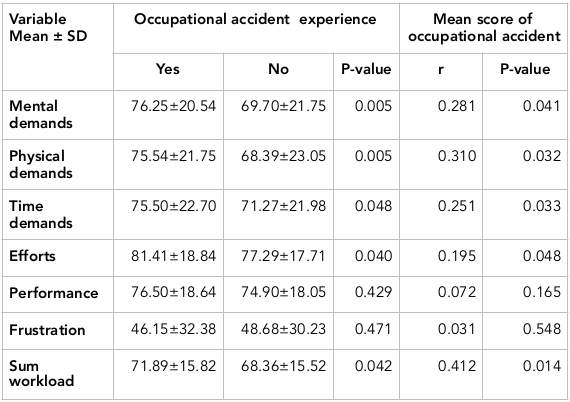
Table 4 shows the correlation between mental workload (and sub-scales) and occupational accidents. According to Table 4 , the mean scores of mental demands, physical demands, time demands, efforts, and sum mental workload in personnel who have experienced occupational accidents were significantly higher compared to personnel without accident experience (p<0.05). Moreover, there was a significant positive correlation of occupational accidents to mental demands (p=0.041), to physical demands (p=0.032), to time demands (p=0.033), to efforts (p=0.048), and to sum mental workload (p=0.014). No significant correlation was observed for occupational accidents with performance (p=0.165) or with frustration (p=0.548).
Discussion
The aim of the current study was to evaluate the correlation between mental workload and occupational accidents in nurses, as well as the factors affecting accidents. The rate of estimated mental workload (69.54 ± 15.71) of the nurses in the study was greater than that for bank staff Giahi et al., 2014, indicating the extent of their mental workload. The estimated amount of mental workload in the current study was lower than the amount reported by Malekpour et al. (2014) for nurses working in the Intensive Care Unit (82.33) and higher than the value reported for nurses working in the Orthopedics Ward (63.5) Malekpour et al., 2014. The difference between these results could possibly be due to the difference between the occupational groups. The population surveyed in the present study was a nursing cadre, while in other studies the participants surveyed were nurses occupying different wards of the hospital.
Evaluation of the sub-scales of mental workload showed that maximum frequency for effort score was 78.61 ± 18.15. This finding implies that nurses consume a lot of energy to carry out their job functions. Zheng et al. (2012) reported that effort score as the highest score of the sub-scales of mental workload Zheng et al., 2012. Additionally, Safari et al. (2013) reported that the sub-scale of mental workload is the highest sub-scale (83.5) for nurses Safari et al., 2013. In our study, the lowest score belonged to frustration (69.54 ± 15.71); this finding concurs with findings from a study by Zheng et al. (2012) Zheng et al., 2012.
There was no significant difference in mental workload in men and women, which corresponds to the study by Malekpour et al. (2014) Malekpour et al., 2014 and Safari et al. (2013) Safari et al., 2013. The job duty for male and female nurses is the same, so there should be no difference. The mean mental workload for the higher aged groups was significantly higher than for the lower aged groups, which may reflect the increase of responsible duties and workload for nurses between 40-50 years of age. Safari et al. (2013) reported a significant correlation between mental workload and age in nurses Safari et al., 2013. Clearly, with increasing age, job concentration and performance may decrease. Thus, the significant correlation between age and mental workload in nurses could be affected by that factor.
Nurses are constantly exposed to stress and burnout Malekpour et al., 2014Morris et al., 2007. This could also affect their mental power. Our results demonstrated that there is no significant correlation between experience and shift hours with workload; other studies have reported an insignificant correlation amongst these variables too Hoonakker et al., 2011Malekpour et al., 2014Safari et al., 2013. The mean of mental workload in personnel with regular shifts was significantly higher than in personnel with erratic shifts. Hoonakker et al. (2011) also reported a significant correlation between shifts and mental workload Hoonakker et al., 2011 and, indeed, shifts have always been considered a key factor for mental workload in a job Costa, 2010.
Studies indicated that there is a significant correlation between tiredness and workload; shift workers with circadian problems or those receiving inadequate rest are more inclined to be tired. The accumulative tiredness could affect overall mental workload Rahimi et al., 2012. The mean number of occupational accidents in the current study was greater than those for the chemical industry Vinodkumar and Bhasi, 2009, indicating that the nursing work environment is a perilous and risky one. The percentage of injured individuals in this study was lower than that reported by McCaughey et al. (2013), which evaluated nurses in hospitals of India. Indeed, the rate of accidents in our current study was greater than McCaughey’s study McCaughey et al., 2013. This indicates that a certain group of people are more inclined to be injured at these hospitals, and it will be useful to identify them immediately.
The number of injured people and rate of accidents for men was significantly higher than for women, which is consistent with observations by Bakhtiyari et al. (2012) Bakhtiyari et al., 2012. The higher rate of accidents among men is conceivable since men typically perform heavy work and movements in the wards. The mean number of accidents in younger and elder groups were significantly greater than that for the middle-age group, which concurs with the study by Ghamari et al. (2013) Ghamari et al., 2013. The main cause of the high rate of accidents in the younger group could be due to less experience and unfamiliarity with dangers of safety in the setting. Thus, the cause of a high rate of accidents in elder group might be due to decreased focus and ability.
There was no significant correlation between hours of work time per week and accidents. This could relate to the equal hours of work time among staff. As aforementioned, the mean number of accidents in nursing wards is significantly higher than other occupational groups. Personnel working in the servicing ward (typically lower education) have less information about necessary actions to take when confronting different situations. Also, they transfer patients and, accordingly, accidents are among the highest in this group than other groups.
Moreover, our results showed that mental workload in nurses who have experienced occupational accidents is greater than that of nurses with no experience. Furthermore, there was a positive correlation between mental workload and mean of accidents. Mazur et al. (2012) reported that there is a significant correlation between radiotherapy accidents and mental workload score Mazur et al., 2012. Additionally, there is a significant correlation between the subscales of mental need, physical need, effort score, and frequency of accidents. If the mental and physical needs of an occupation are high, the staff is obliged to do his/her job duties with greater effort. This affects the thinking process and concentration, and increases the number of errors. Holden et al. (2011) showed that there is a significant positive correlation between mental workload and possibility of creating errors Holden et al., 2011. In fact, human error is one of the major causes of occupational accidents Wiegmann and Shappell, 2001Young et al., 2008.
Correspondingly, Di Stasi et al. (2009) showed that people with higher mental workload tend to exhibit perilous behaviors Di Stasi et al., 2009, which can increase occupational accidents. Nurses are among professionals who are constantly under risk of occupational accidents, such as needle stick injuries, exposure to chemical materials, and acquisition of musculoskeletal injuries Alavi, 2014. The high level of mental workload not only affects occupational accidents but also increases the prevalence of depression, occupational stress, and burnout. Furthermore, the high mental workload affects health and welfare of personnel as well as safety of patients Holden et al., 2011.
Indeed, occupational accidents are affected by various factors, including physical and psychological conditions of the staff, organizational factors (such as organizational culture), and safety conditions. Further studies are needed to investigate the effects of these factors on mental workload and occupational accidents. In the future, it will be important to better understand the factors affecting mental workload and accidents, evaluate more subjects, and possibly investigate the impact of adequate rest at home.
Conclusion
There is a significant positive correlation between mental workload and occupational accidents. Taking actions to prevent or decrease mental workload can possibly lead to a decrease in occupational accidents for nurses.
Author Contribution
Milad Derakhshanjazari and Hamid Salehiniya was all responsible for the study conception and design. Fatemeh Honarjoo performed the sampling and data collection and prepared the draft of the manuscript. Vali sarsangi made critical revisions to the paper for important intellectual content, performed the data analysis and supervised the study. All authors reviewed and commented on final draft.
References
-
A.
Aghajanlou,
Z.K.
NIROUMAND,
B.Z.
Safavi,
M.H.
ALAVI.
Types and rates of occupational accidents in nursing students at nursing and midwifery colleges in Tehran. 2007
.
-
N.M.
Alavi.
Occupational hazards in nursing. Nursing and midwifery studies.
2014;
3
.
-
M.
Bakhtiyari,
A.
Aghaie,
A.
Delpisheh,
S.
Akbarpour,
F.
Zayeri,
H.
Soori,
M.
Salehi,
M.
Arji.
An epidemiologic survey of recorded job-related accidents by Iranian social security organization (2001-2005). Journal of Rafsanjan University of Medical Sciences.
2012;
11
:
231-246
.
-
A.
Cao,
K.K.
Chintamani,
A.K.
Pandya,
R.D.
Ellis.
NASA TLX: software for assessing subjective mental workload. Behavior research methods.
2009;
41
:
113-117
.
-
G.
Costa.
Shiftwork related problems in hospital workers. Giornale italiano di medicina del lavoro ed ergonomia.
2010;
32
:
343-346
.
-
L.L.
Di Stasi,
V.
Álvarez-Valbuena,
J.J.
Cañas,
A.
Maldonado,
A.
Catena,
A.
Antolí,
A.
Candido.
Risk behaviour and mental workload: Multimodal assessment techniques applied to motorbike riding simulation. Transportation research part F: traffic psychology and behaviour.
2009;
12
:
361-370
.
-
R.R.
Gershon,
P.W.
Stone,
M.
Zeltser,
J.
Faucett,
K.
Macdavitt,
S.-S.
Chou.
Organizational climate and nurse health outcomes in the United States: a systematic review. Industrial health.
2007;
45
:
622-636
.
-
F.
Ghamari,
I.
Mohammadfam,
A.
Mohammadbeigi,
H.
Ebrahimi,
M.
Khodayari.
Determination of effective risk factors in incidence of occupational accidents in one of the large metal industries, Arak (2005-2007). Iran Occupational Health.
2013;
9
:
89-96
.
-
M.
Ghasemi,
A.
Zakerian,
M.
Azhdari.
Control of Human Error and comparison Level risk after correction action With the SHERPA Method in a control Room of petrochemical industry. Iran Occupational Health.
2011;
8
:
2-0
.
-
O.
Giahi,
E.
Darvishi,
M.
Akbarzadeh,
S.
Shahsavari.
Assessment of the relationship of the risk of subjective work load to musculoskeletal disorders in bank staff in Kurdistan Province. Scientific Journal of Kurdistan University of Medical Sciences.
2014;
19
:
36-45
.
-
R.J.
Holden,
N.R.
Patel,
M.C.
Scanlon,
T.M.
Shalaby,
J.M.
Arnold,
B.-T.
Karsh.
Effects of mental demands during dispensing on perceived medication safety and employee well-being: A study of workload in pediatric hospital pharmacies. Research in social and administrative Pharmacy.
2010;
6
:
293-306
.
-
R.J.
Holden,
M.C.
Scanlon,
N.R.
Patel,
R.
Kaushal,
K.H.
Escoto,
R.L.
Brown,
S.J.
Alper,
J.M.
Arnold,
T.M.
Shalaby,
K.
Murkowski.
A human factors framework and study of the effect of nursing workload on patient safety and employee quality of working life. Quality and Safety in Health Care.
2011;
20
:
15-24
.
-
P.
Hoonakker,
P.
Carayon,
A.P.
Gurses,
R.
Brown,
A.
Khunlertkit,
K.
McGuire,
J.M.
Walker.
Measuring workload of ICU nurses with a questionnaire survey: the NASA Task Load Index (TLX). IIE transactions on healthcare systems engineering.
2011;
1
:
131-143
.
-
Y.-H.
Huang,
M.
Ho,
G.S.
Smith,
P.Y.
Chen.
Safety climate and self-reported injury: Assessing the mediating role of employee safety control. Accident Analysis & Prevention.
2006;
38
:
425-433
.
-
L.
Kohn,
J.
Corrigan,
M.
Donaldson.
To err is human: building a safer health system. National Academy of Science, Institute of Medicine.
2002;
6
.
-
B.S.
Levy.
Occupational and environmental health: recognizing and preventing disease and injury. Lippincott Williams & Wilkins.
2006
.
-
F.
Malekpour,
Y.
Mohammadian,
A.
Malekpour,
Y.
Mohammadpour,
A.
Sheikh Ahmadi,
A.
Shakarami.
Assessment of mental workload in nursing by using NASA-TLX. Journal of Urmia Nursing And Midwifery Faculty.
2014;
11
:
0-0
.
-
L.M.
Mazur,
P.R.
Mosaly,
M.
Jackson,
S.X.
Chang,
K.D.
Burkhardt,
R.D.
Adams,
E.L.
Jones,
L.
Hoyle,
J.
Xu,
J.
Rockwell.
Quantitative assessment of workload and stressors in clinical radiation oncology. International Journal of Radiation Oncology* Biology* Physics.
2012;
83
:
e571-e576
.
-
D.
McCaughey,
J.L.
DelliFraine,
G.
McGhan,
N.S.
Bruning.
The negative effects of workplace injury and illness on workplace safety climate perceptions and health care worker outcomes. Safety science.
2013;
51
:
138-147
.
-
M.
Mohammadi,
J.
Nasl Seraji,
H.
Zeraati.
Developing and assessing the validity and reliability of a questionnaire to assess the mental workload among ICUs Nurses in one of the Tehran University of Medical Sciences hospitals, Tehran, Iran. J Sch Public Health Inst Public Health Res.
2013;
11
:
87-96
.
-
R.
Morris,
P.
MacNeela,
A.
Scott,
P.
Treacy,
A.
Hyde.
Reconsidering the conceptualization of nursing workload: literature review. Journal of advanced Nursing.
2007;
57
:
463-471
.
-
D.
Neill.
Nursing Workload and the Changing Health Care Environment: A Review of the Literature. Administrative Issues Journal:.
2011;
Education
:
Practice, and Research 1, 132-143
.
-
J.A.
Owens.
Sleep loss and fatigue in healthcare professionals. The Journal of perinatal & neonatal nursing.
2007;
21
:
92-100
.
-
A.
Ozkan,
M.
Ozdevecioglu,
Y.
Kaya,
F.Ö.
Koç.
Effects of mental workloads on depression-anger symptoms and interpersonal sensitivities of accounting professionals. Revista de Contabilidad.
2015;
18
:
194-199
.
-
F.
Rahimi,
R.
Ahangarzadeh,
R.
Baghaei,
A.
Feizi.
Effective factors on the incidence of medication errors in hospital nurses in Besat hospital in Sanandaj city at years of 2011. J Nurs Midwifery College Kurdistan.
2012;
1
:
2-8
.
-
S.
Rubio,
E.
Díaz,
J.
Martín,
J.M.
Puente.
Evaluation of subjective mental workload: A comparison of SWAT, NASA-TLX, and workload profile methods. Applied Psychology.
2004;
53
:
61-86
.
-
S.
Safari,
H.
Mohammadi-Bolbanabad,
M.
Kazemi.
Evaluation Mental Work Load in Nursing Critical Care Unit with National Aeronautics and Space Administration Task Load Index (NASA-TLX). J Health Sys Res.
2013;
9
:
613-619
.
-
M.
Vinodkumar,
M.
Bhasi.
Safety climate factors and its relationship with accidents and personal attributes in the chemical industry. Safety Science.
2009;
47
:
659-667
.
-
D.A.
Wiegmann,
S.A.
Shappell.
Human error analysis of commercial aviation accidents: Application of the Human Factors Analysis and Classification System (HFACS). Aviation, space, and environmental medicine.
2001;
72
:
1006-1016
.
-
G.
Young,
L.
Zavelina,
V.
Hooper.
Assessment of workload using NASA Task Load Index in perianesthesia nursing. Journal of PeriAnesthesia Nursing.
2008;
23
:
102-110
.
-
B.
Zheng,
X.
Jiang,
G.
Tien,
A.
Meneghetti,
O.N.M.
Panton,
M.S.
Atkins.
Workload assessment of surgeons: correlation between NASA TLX and blinks. Surgical endoscopy.
2012;
26
:
2746-2750
.
Comments
Downloads
Article Details
Volume & Issue : Vol 4 No 08 (2017)
Page No.: 1527-1540
Published on: 2017-08-25
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
- HTML viewed - 7568 times
- Download PDF downloaded - 2248 times
- View Article downloaded - 16 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}