

Copyrights: Reza Sabet, Karamatollah Rahmanian, Abdolreza Sotoodeh Jahromi, Abdolhossein Madani, 2018. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: The most common type of neuropathy in adults is carpal tunnel syndrome (CTS) which is caused by compression of the median nerve at the wrist.
Methods: This quasi-experimental study was conducted to determine the efficacy of gabapentin on nerve conduction studies in patients with mild CTS. The patients with mild CTS were randomly allocated into two groups. Group A received naproxen alone (500 mg/day, orally) while group B received both gabapentin (100-300 mg) and naproxen (500 mg/day, orally) for two months. Sensory nerve conduction velocity (SNCV) and distal motor latency (DML) were performed at baseline and two months after treatment.
Results: There were no significant differences between the two groups with regards to the outcome parameters before initiation of intervention. The SNCV and DML showed no significant improvements in group A (p>0.05), whereas for group B the SNCV and DML of the median nerve were significantly improved at two months after treatment (p<0.001).
Conclusion: Gabapentin was found to be effective for SNCV and DML in patients with mild CTS over a two-month period.
Introduction
The most common type of neuropathy in adults is carpal tunnel syndrome (CTS) caused by compression of the median nerve at the wrist. The prevalence of CTS in the general population, in 2012, was near 3-3.8% Ibrahim et al., 2012. A higher prevalence was reported in women and in manual workers Tseng et al., 2012. Some modalities such as conservative treatment, topical injections and surgery have been used for treatment of CTS Jin et al., 2012. However, the efficacy of these treatments is limited and recurrence of symptoms is common Huisstede et al., 2010.
Current literature demonstrate a trend towards recommending early surgery for CTS cases with or without median nerve denervation, although the American Academy of Orthopedic Surgeons guideline recommends early surgical treatment only for cases with denervation Ono et al., 2010. CTS affects nerve conduction studies with entrapment of the median nerve. Some modalities like local corticosteroid injection Deniz et al., 2012 and surgical decompression can significantly improve nerve conduction studies. Hui et al. suggested that surgical decompression resulted in greater improvement in median nerve conduction velocity than a single injection of steroid Hui et al., 2005.
Gabapentin is an antiepileptic drug and structurally related to Gama-Amino Butyric Acid (GABA). Gabapentin action include high affinity binding to calcium channels and alteration of neurotransmitter release and blood serotonin levels Taylor et al., 1998. Gabapentin is used in a variety of neuropathic pain conditions such as diabetic neuropathy, post herpetic neuralgia, and spinal cord injury Sabet et al., 2017Serpell, 2002. The safety and tolerability of this drug were reported by researchers Hui et al., 2011. However, the studies on effects of gabapentin on nerve conduction studies have been limited. Gabapentin may close chloride channels and open calcium channels in neural cells, as well as change ion flow by membrane channels. Thus, these lead to decreased inhibitory post-synaptic potential and increased speed flow in neural cells. Taverner et al. reported that after a 6-month followup of patients with CTS treated with 1800 mg/day of gabapentin, 5.3% and 26.3% patients showed improvement and normal electromyography findings, respectively Taverner et al., 2008.
This study aims to evaluate the efficacy of gabapentin on sensory nerve conduction velocity (SNCV) and distal motor latency (DML) in patients with mild CTS.
Materials - Methods
This quasi-experimental study was done on 50 consecutive patients with mild CTS (39 women and 11 men, aged 25-59 (41.84±6.88) years) who were randomly divided into two groups. The study protocol was approved by the local ethics committee of Jahrom University of Medical Sciences Jahrom (Jahrom, Iran), and informed consents were obtained from all study participants.
Diagnosis of CTS was based on the clinical and electrophysiological methods. Clinical diagnosis of CTS was done by Boston carpal tunnel questionnaire (BCTQ) which has been validated in other studies Heybeli et al., 2002. The BCTQ has two subscales evaluating the symptom severity scale (SSS) and functional status scale (FSS). The SSS evaluates symptoms such as pain, numbness, weakness, paresthesia, or clumsiness using 11 questions. Five answers are possible to each question; they are scored 1 to 5 according to the severity of symptoms. All answers were summed and the mean scores were calculated. Electrophysiological diagnosis of CTS was based on the criteria proposed by the American Academy of Neurology (1993). Nerve conduction studies were done in the median nerve by standard technique and surface electrodes, and were performed utilizing a EMG-NCV machine (Negar Andishan, Iran).
The median SNCV was measured first by placing a recording electrode on the base of the long finger. Then, the median nerve was stimulated at the wrist 14 cm proximal to the recording electrode. The median SNCV and DML were measured by placing a surface electrode on the muscle belly of the abductor pollicis brevis, stimulating the median nerve at the wrist 7 cm proximal to the electrode. Note that according to the classification by Padua et al., mild carpal tunnel syndrome is recognized when the DML is normal and SNCV is reduced Padua et al., 1997. The SSS score of <3, electrodiagnostic criteria of SNCV ≤40 meter/second (m/s), and distal motor latency <4.4 milliseconds (ms) can indicate mild CTS.
Patients in group A received oral naproxen at a dose of 500 mg/day. Patients in group B received combination therapy of naproxen (500 mg/day) and gabapentin (started at 100 mg/day initially and patients were advised to attend the clinic after the first week of treatment for titrating the drug dose). The drug dosage of gabapentin was titrated to a maximum of 300 mg/day according to the tolerance of patients. Patients were asked to report or visit the clinic if any adverse effects appeared during the study period. If patient did not tolerate the side effects, he or she was excluded from the study.
Patients with mild CTS for more than 3 months were included in the study. Patients with the following conditions were excluded: thenar muscle atrophy, topical steroid injection at wrist in the last 3 months, CTS surgery, pregnant and lactating women, hypersensitivity to gabapentin or non-steroidal anti-inflammatory drugs, renal failure, history of narcotic or alcohol abuse, cervical radiculopathy, and discopathy.
SSS scoring by BCTQ and nerve conduction studies were done before and at 2 months after the start of drug therapy. After the performance of normality tests, the differences from baseline values were compared by paired Student’s t-test; comparisons of changes between two groups were made by independent Student’s t-test. The level of statistical significance was p<0.05.
Results
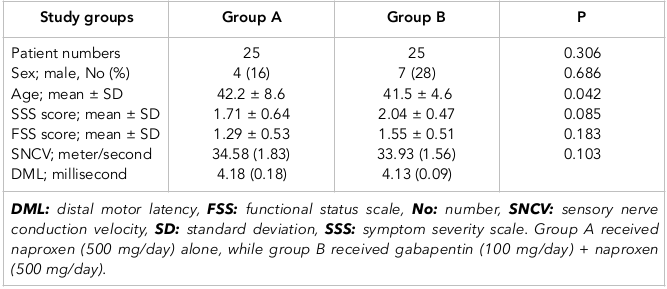
There were no significant differences in terms of age and sex between the two study groups ( Table 1 ). The SSS score of group B before intervention was significantly higher than that for group A (p=0.042), but the FSS score was not significantly different between the two groups before treatment. Also, there was no significant difference in SNCV and DML between the two study groups (p>0.05). No participants were lost in follow-up.
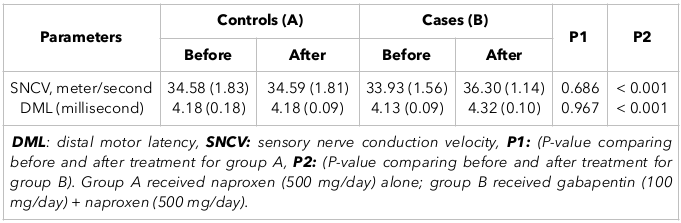
The mean SNCV increased 2.37 m/s two months after combination therapy with gabapentin + naproxen (p<0.001). Also, DML changed significantly after initiation of gabapentin + naproxen (p<0.001). However, SNCV and DML showed no significant change in group A (p>0.05) ( Table 2 ).
Discussion
Our study shows the efficacy of gabapentin on improving SNCV and DML in patients with mild CTS. Gabapentin has been shown to provide significant analgesia in several neuropathic pain conditions, including trigeminal neuralgia and peripheral diabetic neuropathy; it may also be effective in treating neuropathic pain refractory to other anti-epileptic drugs Nicholson, 2000. Some studies evaluated the efficacy of gabapentin in the symptomatic treatment of CTS Taverner et al., 2008. However, the studies that have evaluated the efficacy of gabapentin on SNCV and DML have been limited.
In a study conducted by Eftekharsadat et al. Eftekharsadat et al., 2015, 90 consecutive patients with mild and moderate CTS were randomly divided into 3 groups (A, B and C). For a period of 2 months, Group A received gabapentin (100 mg/day), Group B received gabapentin (300 mg/day), and group C received no treatment. There were no significant changes in (CMAP) and sensory nerve action potential between the groups. Yet, Taverner et al. reported that after a 6-month followup of patients with CTS treated initially with 1800 mg/day of gabapentin, 5.3% and 26.3% patients showed improvement as well as normal electromyography, respectively Taverner et al., 2008.
The recommended dose of gabapentin in patients is 900-3600 mg/day. We initiated the treatment of patients with a dosage of 100 mg/day and increased up to 300 mg/day, according to the patient's tolerance and requirement. Our study shows that gabapentin improved SNCV and DML over baseline and compared to naproxen treatment of patients with mild CTS. Gabapentin may function in closing chloride channels and opening calcium channels in neural cells. Furthermore, it may alter the ion flow in membrane channels, therefore leading to decreased inhibitory post-synaptic potential and increased speed flow in neural cells.
Other modalities such as local corticosteroid injection Deniz et al., 2012 and surgical decompression Evcik et al., 2007 can significantly improve SNCV and the sensory nerve action potential amplitude of the median nerve. However, others have reported no improvement Gurcay, et al. 2009. Deniz et al. suggested that single injection of dexamethasone sodium phosphate significantly improves sensory and motor nerve conduction values when compared to baseline values Deniz et al., 2012. Also, Karadas et al. Karadas et al., 2012 suggested that injection of triamcinolone acetonide once a week and 1% procaine hydrochloride twice a week for 2 weeks can significantly improve electrophysiological findings.
The major limitation of this study was not determining the long-term efficacy of gabapentin on nerve conduction studies in the CTS patients. Other limitations are that patients with moderate or severe CTS were not studied, and there was a low number of participants. In addition, the SSS score was significantly different between the two study groups.
Conclusion
Carpal tunnel syndrome is caused by compression of the median nerve within the carpal tunnel. Our study showed that gabapentin improved the SNCV and DML. Thus, mild CTS cases may be good candidates for treatment with gabapentin.
Abbreviations
BCTQ: Boston Carpal Tunnel Questionnaire
CTS: Carpal Tunnel Syndrome
DML: Distal Motor Latency
FSS: Functional Status Scale
GABA: Gama-Amino Butyric Acid
SD: Standard Deviation
SNCV: Sensory Nerve Conduction Velocity
SSS: symptom severity scale
Author Contribution
Reza Sabet: Design of study, Patients managements, proposal of study writing, final content of study; Karamatollah Rahmanian: proposal of study writing, interpretation, final content of study; Abdolreza Sotoodeh Jahromi, Abdolhossein Madani: proposal of study writing, enrolled data, manuscript writing.
References
-
[No authors listed].
Report of the Quality Standards Subcommittee of the American Academy of Neurology. Practice parameter for carpal tunnel syndrome (summary statement). Neurology.
1993;
43(11)
:
2406-2409
.
-
O.
Deniz,
R.
Aygül,
D.
Kotan,
G.
Ozdemir,
F. O.
Odabaş,
M. D.
Kaya,
H.
Ulvi.
The effect of local corticosteroid injection on F-wave conduction velocity and sympathetic skin response in carpal tunnel syndrome. Rheumatology International.
2012;
32(5)
:
1285-1290
.
View Article PubMed Google Scholar -
B.
Eftekharsadat,
A.
Babaei-Ghazani,
A.
Habibzadeh.
The Efficacy of 100 and 300 mg Gabapentin in the Treatment of Carpal Tunnel Syndrome. Iranian Journal of Pharmaceutical Research.
2015;
14(4)
:
1275-1280
.
PubMed Google Scholar -
D.
Evcik,
V.
Kavuncu,
T.
Cakir,
V.
Subasi,
M.
Yaman.
Laser therapy in the treatment of carpal tunnel syndrome: A randomized controlled trial. Photomedicine and Laser Surgery.
2007;
25(1)
:
34-39
.
View Article PubMed Google Scholar -
E.
Gurcay,
E.
Unlu,
A. G.
Gurcay,
R.
Tuncay,
A.
Cakci.
Evaluation of the effect of local corticosteroid injection and anti-inflammatory medication in carpal tunnel syndrome. Scottish Medical Journal.
2009;
54(1)
:
4-6
.
View Article PubMed Google Scholar -
N.
Heybeli,
S.
Kutluhan,
S.
Demirci,
M.
Kerman,
E. F.
Mumcu.
Assessment of outcome of carpal tunnel syndrome: A comparison of electrophysiological findings and a self-administered Boston questionnaire. Journal of Hand Surgery (Edinburgh.
2002;
Lothian)
:
27(3)
.
View Article PubMed Google Scholar -
A. C.
Hui,
S.
Wong,
C. H.
Leung,
P.
Tong,
V.
Mok,
D.
Poon,
R.
Boet.
A randomized controlled trial of surgery vs steroid injection for carpal tunnel syndrome. Neurology.
2005;
64(12)
:
2074-2078
.
View Article PubMed Google Scholar -
A. C.
Hui,
S. M.
Wong,
H. W.
Leung,
B. L.
Man,
E.
Yu,
L. K.
Wong.
Gabapentin for the treatment of carpal tunnel syndrome: A randomized controlled trial. European Journal of Neurology.
2011;
18(5)
:
726-730
.
View Article PubMed Google Scholar -
B. M.
Huisstede,
P.
Hoogvliet,
M. S.
Randsdorp,
S.
Glerum,
M.
van Middelkoop,
B. W.
Koes.
Carpal tunnel syndrome. Part I: Effectiveness of nonsurgical treatments—a systematic review. Archives of Physical Medicine and Rehabilitation.
2010;
91(7)
:
981-1004
.
-
I.
Ibrahim,
W. S.
Khan,
N.
Goddard,
P.
Smitham.
Carpal tunnel syndrome: A review of the recent literature. The Open Orthopaedics Journal.
2012;
6(1)
:
69-76
.
View Article PubMed Google Scholar -
G. Q.
Jin,
J.
Yang,
C. Y.
Li,
X. F.
Ming,
X. F.
Zhao,
C. S.
Cheng.
Treatment of carpal tunnel syndrome with mini-incision decompression. Zhongguo Gu Shang.
2012;
25(1)
:
58-61
.
PubMed Google Scholar -
O.
Karadaş,
O. K.
Omaç,
F.
Tok,
A.
Ozgül,
Z.
Odabaşi.
Effects of steroid with repetitive procaine HCl injection in the management of carpal tunnel syndrome: An ultrasonographic study. Journal of the Neurological Sciences.
2012;
316(1-2)
:
76-78
.
View Article PubMed Google Scholar -
B.
Nicholson.
Gabapentin use in neuropathic pain syndromes. Acta Neurologica Scandinavica.
2000;
101(6)
:
359-371
.
View Article PubMed Google Scholar -
S.
Ono,
P. J.
Clapham,
K. C.
Chung.
Optimal management of carpal tunnel syndrome. International Journal of General Medicine.
2010;
3
:
255-261
.
PubMed Google Scholar -
L.
Padua,
M.
LoMonaco,
B.
Gregori,
E. M.
Valente,
R.
Padua,
P.
Tonali.
Neurophysiological classification and sensitivity in 500 carpal tunnel syndrome hands. Acta Neurologica Scandinavica.
1997;
96(4)
:
211-217
.
View Article PubMed Google Scholar -
R.
Sabet,
K.
Rahmanian,
A.S.
Jahromi,
A.
Madani.
Analgesic effect of gabapentin in patients with carpal tunnel syndrome. Journal of Applied Pharmaceutical Science.
2017;
7
:
079-082
.
-
M. G.
Serpell,
the Neuropathic pain study group.
Gabapentin in neuropathic pain syndromes: A randomised, double-blind, placebo-controlled trial. Pain.
2002;
99(3)
:
557-566
.
View Article PubMed Google Scholar -
D.
Taverner,
M. P.
Lisbona,
N.
Segalés,
E.
Docampo,
J.
Calvet,
S.
Castro,
P.
Benito.
Efficacy of gabapentin in the treatment of carpal tunnel syndrome. Medicina Clínica.
2008;
130(10)
:
371-373
.
View Article PubMed Google Scholar -
C.P.
Taylor,
N.S.
Gee,
T.Z.
Su,
J.D.
Kocsis,
D.F.
Welty,
J.P.
Brown,
D.J.
Dooley,
P.
Boden,
L.
Singh.
A summary of mechanistic hypotheses of gabapentin pharmacology. epilepsy research.
1998;
29
:
233-249
.
-
C. H.
Tseng,
C. C.
Liao,
C. M.
Kuo,
F. C.
Sung,
D. P.
Hsieh,
C. H.
Tsai.
Medical and non-medical correlates of carpal tunnel syndrome in a Taiwan cohort of one million. European Journal of Neurology.
2012;
19(1)
:
91-97
.
View Article PubMed Google Scholar
Comments
Downloads
Article Details
Volume & Issue : Vol 5 No 1 (2018)
Page No.: 1923-1930
Published on: 2018-01-19
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 28889 times
- Download PDF downloaded - 2141 times
- View Article downloaded - 0 times

{kind=link}
{kind=link}