

Copyrights: Ruqiya Pervaiz, Özlem Ercantan, 2018. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: The aim of this study was to investigate the correlation between mortality from non-communicable diseases (NCDs) and national human development index (HDI) of a country, as well as investigate the correlation between premature mortality from NCDs and national HDI.
Method: Data for age-standardized mortality rate (ASRM) of NCDs and premature mortality (before age 70 years) in percentage for total NCDs in 2015 were obtained from the World Health Organization (WHO) databases. National HDI data for the year 2015 were obtained from the 2015 Human Development Report. Linear regression model was used for assessment of correlation between HDI and mortality. One-way ANOVA was used to test the difference in mean mortality of various HDI group countries; P ≤ 0.05 was considered significant.
Results: The results suggested an inverse correlation between HDI and ASRM for both men and women. The negative relation was also reported for percentage premature mortality and HDI. Tukey post hoc test (p < 0.001) indicated that countries with very high HDI have low ASRM and premature mortality (compared to those with high HDI and so on). The greatest mortality was observed in low HDI countries.
Conclusion: Management of non-communicable diseases is one of the greatest challenges for low and middle HDI countries. In order to control the disease burden, governments should pay serious attention to their economic development.
Introduction
Non-communicable diseases (NCDs) are the leading cause of death worldwide. NCDs comprise cardiac diseases, stroke, diabetes, respiratory diseases, and cancer WHO, 2015. Among these, the fraction of highest mortality is attributed to cardiovascular diseases, followed by cancer, chronic obstructive pulmonary disease, and diabetes (Murray et al., 2012).
The common risk factors for the top four NCDs (cardiovascular disease, cancer, diabetes, and chronic pulmonary diseases) are smoking, alcohol use, lack of physical activity Lozano et al., 2012, and unhealthy diet Pervaiz et al., 2017. About 80% of deaths from NCDs result from the above 4 diseases Lozano et al., 2012.
According to the estimations of the WHO, NCDs are responsible for 36 million deaths in 2008, which represents 63% of all WHO, 2011. Approximately 80% of these NCD-related mortalities are reported in middle and low Human Development Index (HDI) countries with a high proportion of premature mortality before age 60 WHO, 2013. By 2020, NCDs are predicted to account for 80% of the global burden of diseases; more than two-thirds of deaths will be in developing countries and half of the deaths will be premature deaths (under 70 years of age) according to the WHO data WHO, 2013.
Moreover, according to the WHO estimation, in the next ten years, 17% increase in the global burden of NCDs WHO, 2013. NCDs account for almost half of all deaths in Asia, and represent 47% of the global disease burden WHO, 2013. In developing countries, the mortality of NCDs is very high; for instance, cardiovascular disease and diabetes account for 80% of mortality cases, chronic lung diseases account for 90%, and two-thirds of all cancer deaths are reported from developing countries Hancock et al., 2011.
NCDs are obstacles to socioeconomic development Beaglehole et al., 2011. In developing countries, people are more exposed to behavioral risk factors arising from poverty; consequently, poverty increases due to NCDs Beaglehole & Yach, 2003.
We aim to investigate the correlation between the socioeconomic status of countries and NCD-associated mortality as well as between premature mortality under age 70 years (expressed as % of all NCDs).
Methods
Data Acquisition
The ASRM of NCD and premature mortality in percentage of total NCD WHO, 2015 for 2015 were obtained from the World Health Organization (WHO) databases for 183 countries. Data for National HDI for 2015 were obtained from the Human Development Report 2015 Jahan et al., 2015. All data were obtained for 183 countries in the world. These countries were categorised into four groups on the basis of HDI. Three parameters (i.e. life expectancy at birth, mean years and expected years of schooling, and gross national income per capita) collectively comprise the HDI. The values range from 0 to 1 and there are four categories (Low HDI < 0.536, medium HDI 0.536-0.711, high HDI 0.712-0.804, and very high HDI ≥ 0.805). These countries of the world were classified into the above four categories.
Analysis
Linear regression model was used for the assessment of correlation between HDI and NCD-related mortality (ASRM and premature mortality % of all NCDs). One-way ANOVA is used to test the difference in mean mortality of the four different HDI groups countries; P ≤ 0.05 is considered significant. SPSS version 20 was used for all statistical analyses.
Results
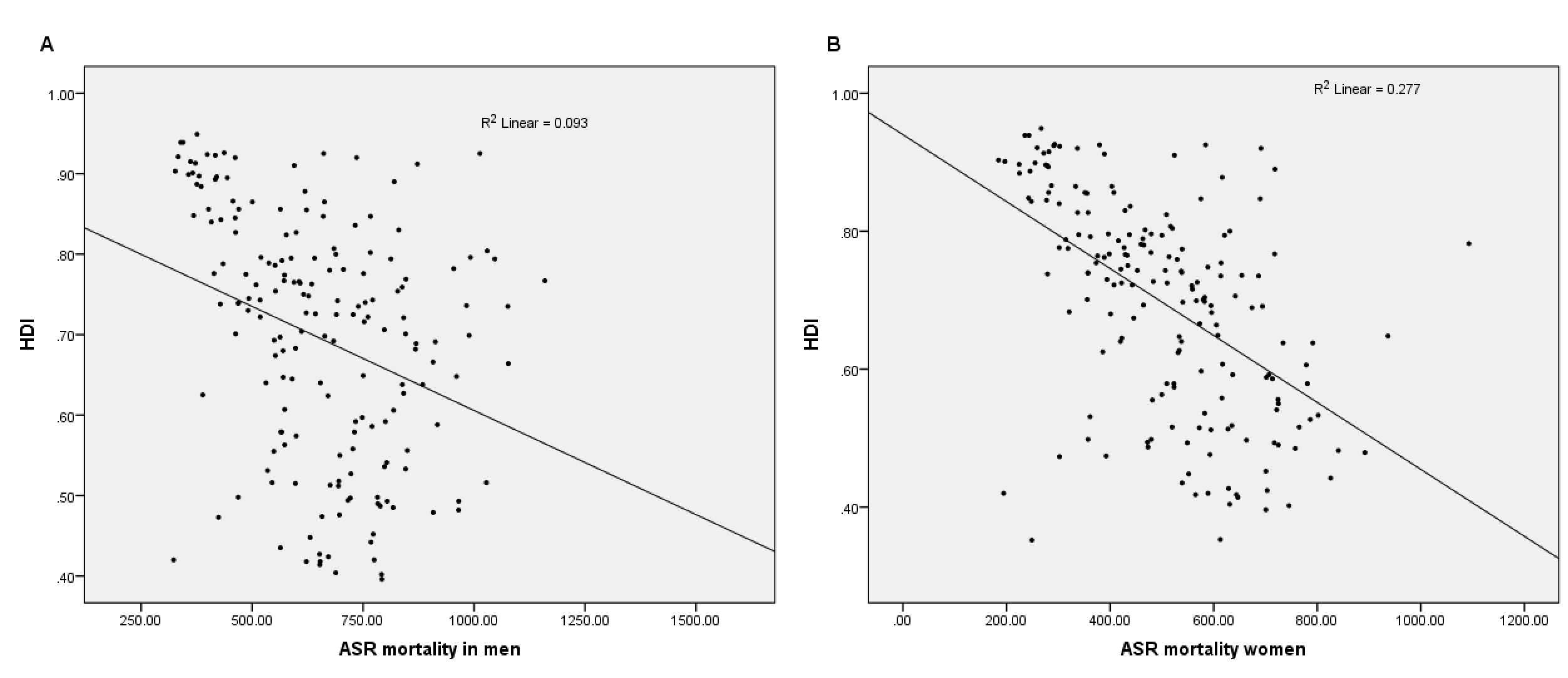
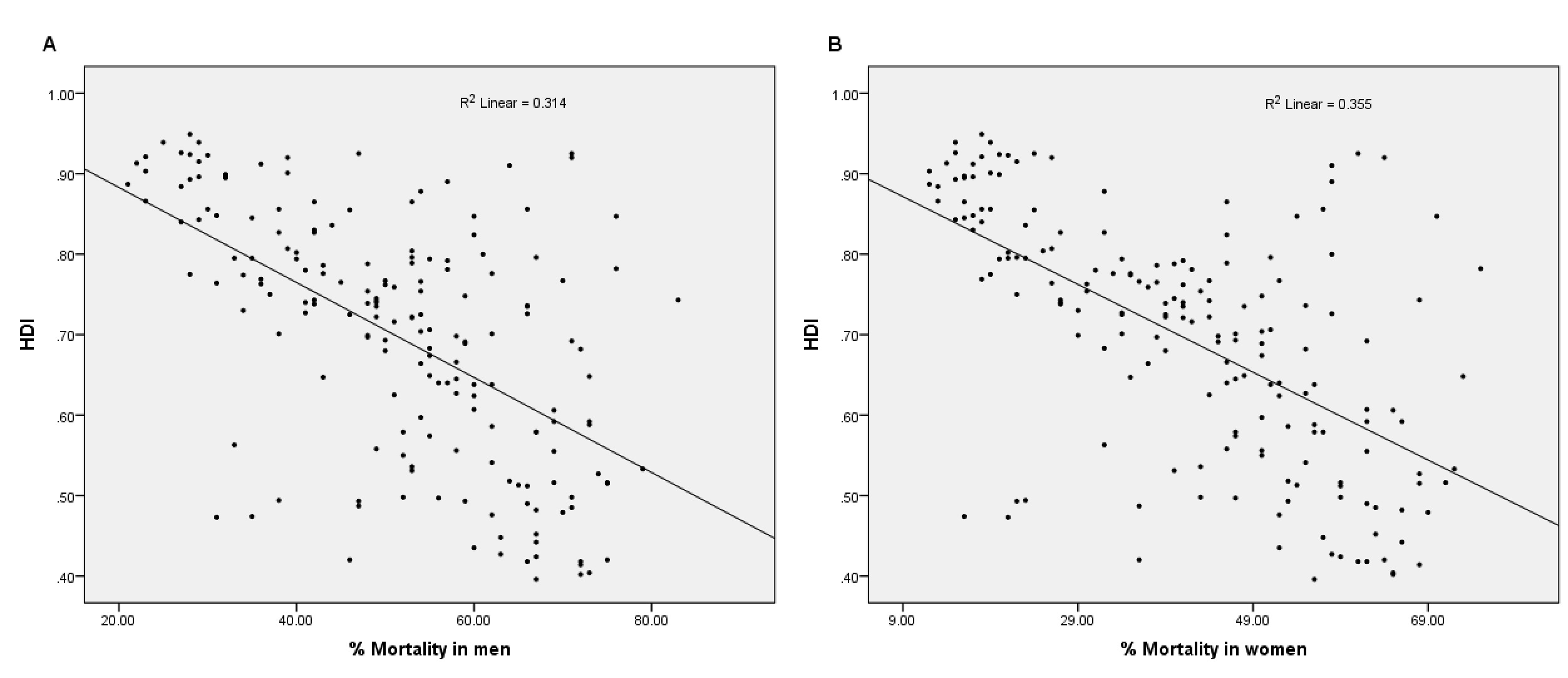
Pearson correlation suggested an inverse correlation between HDI and ASRM in both men (r =-0.305; p<0.001) and women (r=-0.526; p<0.001). Negative correlation was also reported for % of premature mortality and HDI (r=-0.560; p<0.001 for men; r =-0.596; p <0.001 for women).
Correspondingly, linear regression analysis also demonstrated a negative effect of HDI on ASRM (adjusted R2=0.093, β =-0.305, p<0.001 for men and adjusted R2 =0.273, β =-0.526, p<0.001) ( Figure 1A , Figure 1B ). In addition, there was negative effect of HDI on % premature mortality (adjusted R2=0.314, β=-0.560, p<0.001 for men; adjusted R2=0.355, β=-0.596, p<0.001 for women) ( Figure 2A , Figure 2B ).
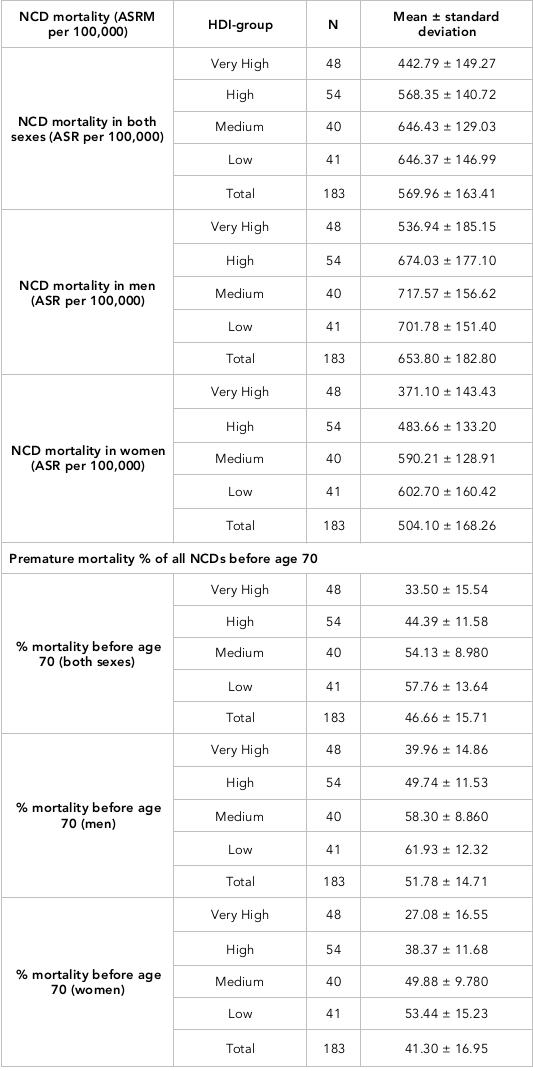
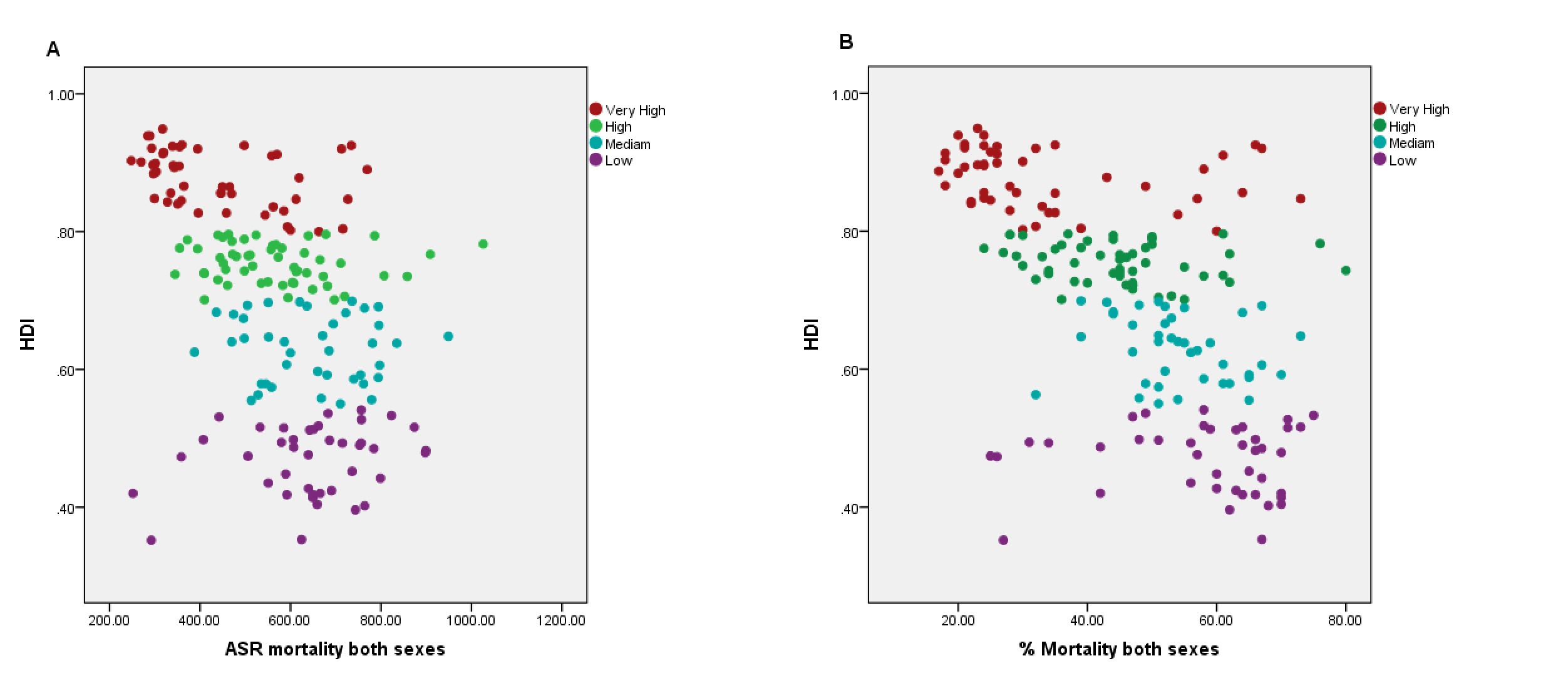
Tukey post hoc test (p < 0.001) demonstrated that countries with very high HDI have low ASRM and premature mortality than those with high HDI and so on. The highest mortality rate was indicated in low HDI countries ( Table 1 ) ( Figure 3A , Figure 3B ).
Discussion
The results from 183 countries in the world indicated an inverse correlation between NCD-related mortality and HDI. Likewise, it was shown that HDI is inversely related with NCD-associated premature mortality. There is a direct correlation between ASRM and premature mortality (r=0.719, p>0.001). The highest NCD mortality was reported in medium and low HDI countries.
Previous studies have suggested that in high-income countries the proportional mortality from NCD is higher than low and middle HDI countries. The reason for this is that low mortality rates from infectious diseases, and mother and child death rates, are prevalent in the higher income countries. Nevertheless, the absolute number of mortality from NCD is higher in the middle and low HDI countries due to a larger population in these countries. Similarly, the ASRM from NCD in these low and middle HDI countries is high WHO, 2011.
Cardiovascular diseases are the primary cause of death globally (Murray et al., 2012). The ASRM from cardiovascular diseases declined since the 1980s, with the most remarkable decline in high-income countries such as North America, Western Europe, and Australia. While in South Asia and former Soviet Union countries, the ASRM increased in the 1990s and decreased after 2000. Central Asia and Eastern Europe had their highest cardiovascular disease mortality in 2010. On average, higher premature mortality of cardiovascular diseases was reported in South Asia, North Africa, the Middle East, and Sub-Saharan Africa Moran et al., 2014.
Cancer is the second most common cause of death globally after cardiovascular diseases (Murray et al., 2012). County-wide studies have indicated an increasing trend of cancer incidence Pervaiz et al., 2017. The mortality to incidence ratio of cancer is highest in the low and medium income countries of Africa Pervaiz & Faisal, 2017 as well as in other parts of the world Bray et al., 2012.
Conclusion
It is concluded that NCDs represent the largest health burden in low and medium HDI countries. Governments and stakeholders in low- and-medium- HDI countries should make serious efforts in improving economic development in order to control NCDs, which have become a major global health concern.
Abbreviations
ANOVA: Analysis of variance
ASRM: Age-standardized mortality rate
HDI: Human development index
NCDs: Non-communicable diseases
SPSS: Statistical Package for Social Sciences
WHO: World Health Organization
Author Contribution
RP participated in the conception of the study, data acquisition, interpretation and drafting the manuscript. ÖE critically revised the article for important intellectual content.
References
-
R.
Beaglehole,
D.
Yach.
Globalisation and the prevention and control of non-communicable disease: The neglected chronic diseases of adults. Lancet.
2003;
362(9387)
:
903-908
.
View Article PubMed Google Scholar -
R.
Beaglehole,
R.
Bonita,
R.
Horton,
C.
Adams,
G.
Alleyne,
P.
Asaria,
J.
Watt,
the NCD Alliance.
the Lancet NCD Action Group.
Priority actions for the non-communicable disease crisis. Lancet.
2011;
377(9775)
:
1438-1447
.
View Article PubMed Google Scholar -
F.
Bray,
A.
Jemal,
N.
Grey,
J.
Ferlay,
D.
Forman.
Global cancer transitions according to the Human Development Index (2008-2030): A population-based study. The Lancet. Oncology.
2012;
13(8)
:
790-801
.
-
A. J.
Ferrari,
F. J.
Charlson,
R. E.
Norman,
S. B.
Patten,
G.
Freedman,
C. J.
Murray,
H. A.
Whiteford.
Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Medicine.
2013;
10(11)
:
e1001547
.
View Article PubMed Google Scholar -
World Health Organization.
Global status report on noncommunicable diseases 2011. Geneva: World Health Organization (http://www.who.int/nmh/publications/ncd_report2010/en).
2011
.
-
C.
Hancock,
L.
Kingo,
O.
Raynaud.
The private sector, international development and NCDs. Globalization and Health.
2011;
7(1)
:
23
.
View Article PubMed Google Scholar -
S.
Jahan,
E.
Jespersen,
S.
Mukherjee,
M.
Kovacevic,
A.
Bonini,
C.
Calderon,
S.
Lucic.
Human development report 2015: Work for human development. New York, NY, USA: UNDP.
2015
.
-
R.
Lozano,
M.
Naghavi,
K.
Foreman,
S.
Lim,
K.
Shibuya,
V.
Aboyans,
Z. A.
Memish.
Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet.
2012;
380(9859)
:
2095-2128
.
View Article PubMed Google Scholar -
A. E.
Moran,
M. H.
Forouzanfar,
G.
Roth,
G.
Mensah,
M.
Ezzati,
C. J.
Murray,
M.
Naghavi.
Temporal trends in ischemic heart disease mortality in 21 world regions, 1980-2010: The Global Burden of Disease 2010 Study. Circulation, CIRCULATIONAHA-113.
2014
.
-
World Health Organization.
Noncommunicable diseases. Geneva: World Health Organization, 2013 (http://www.who.int/mediacentre/factsheets/fs355/en/).
2013
.
-
R.
Pervaiz,
F.
Faisal.
Cancer incidence and mortality are associated with human development index and health setups in Africa. Journal of the Egyptian National Cancer Institute.
2017;
29(3)
:
123-126
.
View Article PubMed Google Scholar -
R.
Pervaiz,
P.
Tulay,
F.
Faisal,
N.
Serakinci.
Incidence of cancer in the Turkish Republic of Northern Cyprus. Turkish Journal of Medical Sciences.
2017;
47(2)
:
523-530
.
View Article PubMed Google Scholar -
World Health Organization.
Non-communicable diseases, http://www.who.int/gho/ncd/mortality_morbidity/ncd_total/en/. Accessed on 25th may 2017. World Health Organization.
2015
.
-
World Health Organization.
Non-communicable diseases, http://www.who.int/gho/ncd/mortality_morbidity/ncd_premature/en/. Accessed on 25th may 2017. World Health Organization.
2015
.
-
World Health Organization.
Cause-specific mortality, 2008: WHO region by country. Geneva: WHO.
2011
.
-
World Health Organization.
Global action plan for the prevention and control of non-communicable diseases 2013-2020. World Health Organization.
2013
.
Comments
Downloads
Article Details
Volume & Issue : Vol 5 No 1 (2018)
Page No.: 1967-1974
Published on: 2018-01-26
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
- HTML viewed - 17824 times
- Download PDF downloaded - 2642 times
- View Article downloaded - 0 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}