

Copyrights: Mehboob Alam, Muhammad Khan, Syed Imran Ahmed, Syed Shahzad Ali, 2018. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Objective: To compare the effectiveness of neural mobilization and ultrasound therapy on pain severity in carpal tunnel syndrome (CTS).
Methods: This randomized controlled trial was conducted on 48 CTS patients at the Physiotherapy Department IPM&R, DUHS between 23rd January 2017 and 22nd July 2017. The CTS patients were randomly allocated into 2 equal groups by simple randomization method. Group 1 received neural mobilisation; Group 2 received ultrasound therapy with a predetermined intensity. A total of 12 sessions were given over a period of 4 weeks. Pre and post intervention data were collected from both groups on Visual Analogue Scale (VAS) to measure pain. SPSS version 20 was used for data analysis. Comparisons between post test results of both groups were done by using paired sample t-test with a p-value < 0.05 considered as significant.
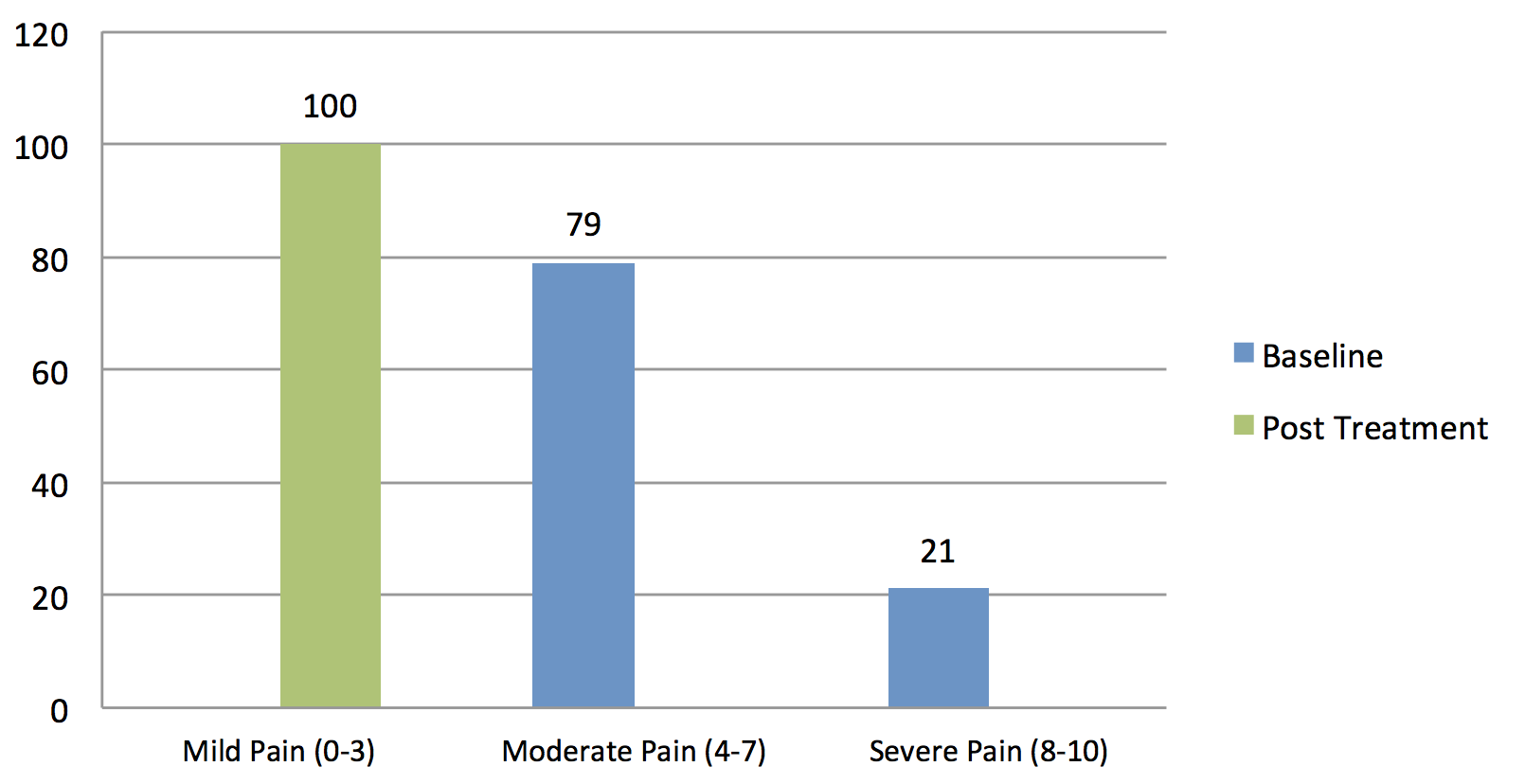
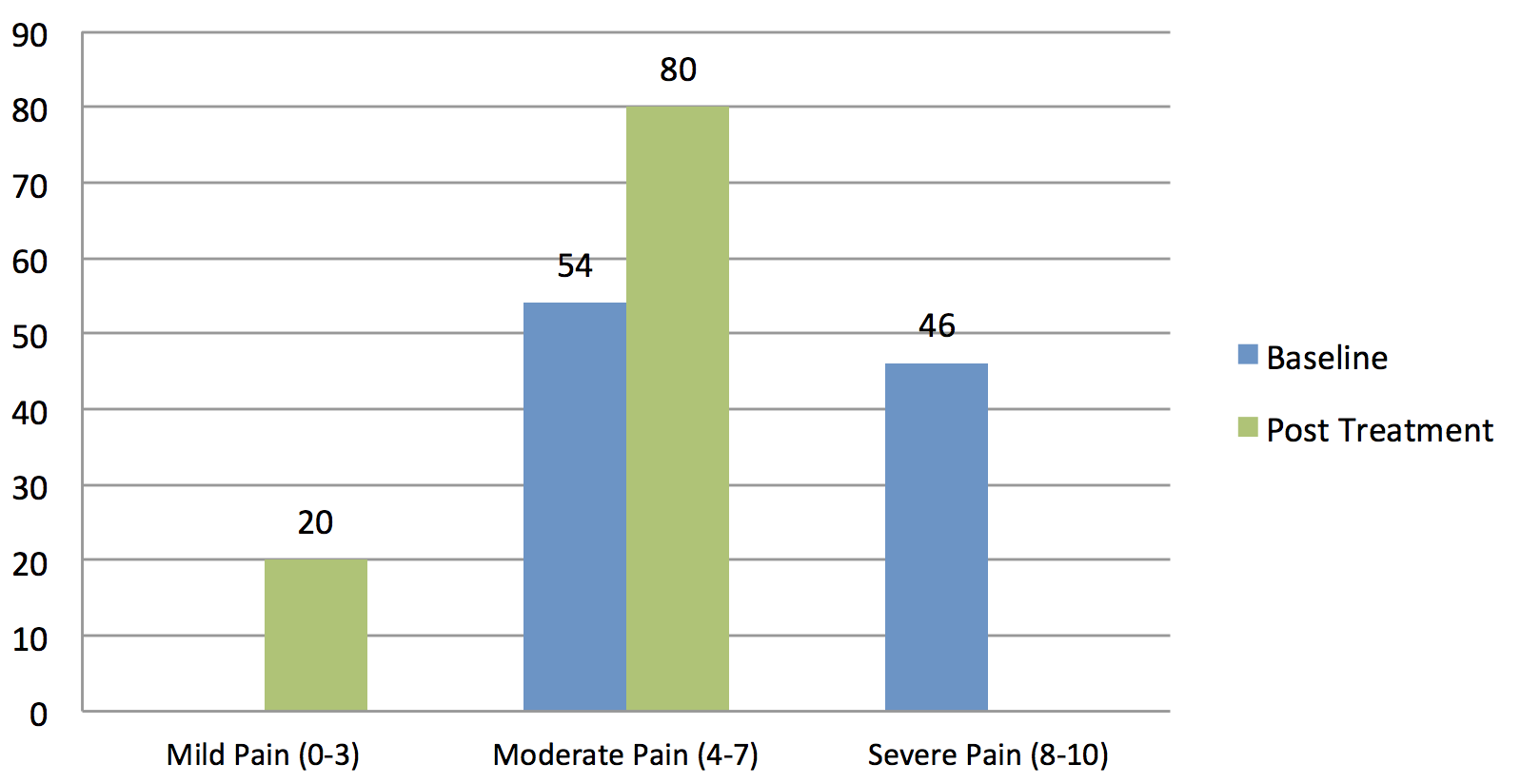
Results: It was found that the 79% (19 cases) and 21% (5 cases) in Group 1 (Neural Mobilization), who prior to the treatment had faced moderate and severe pain, respectively, all experienced successful treatment. Indeed, after treatment 100% (24) of the cases only experienced mild pain, indicating successful treatment. For Group 2 (Ultrasound Therapy), 54% (13) and 46% (11) of cases were with moderate and severe pain before treatment; after administering the treatment 20% (5 cases) had mild pain and 80% (19 cases) had moderate pain.
Conclusion: Neural mobilization for median nerve is more beneficial than ultrasound therapy in reducing pain intensity and functional limitations due to CTS.
Background
Carpal Tunnel Syndrome (CTS) is a clinical condition that results from median nerve compression at the wrist, causing disabling pain which leads to limitations in daily life activities, discomfort and sleep disturbance [1]. The cause of CTS is unknown; however, oral contraceptives, obesity, arthritis, diabetes, hypothyroidism and/or local trauma have been documented as causes in studies [2]. A report that was based on electrophysiological testing suggested that 20% of CTS patients complained of pain, tingling sensation, numbness, and weakness around the wrists and hands [3]-[5] . Occupational groups such as carpenters, musicians, dentists, shoemakers, butchers, tailors, computer operators, and clerks are at high risk for CTS due to repetitive hand movements. A high incidence of CTS has also been reported in laboratory workers as their work requires usage of both hands for about 4- 6 hours a day . Several conventional therapies are available for the management of CTS. These include steroid injections, night splints, ultrasound therapy, manual therapy, acupuncture, yoga exercises, and soft tissue mobilization. A study, by Page et al., discussed that in CTS two nerves are compressed which results in pain and numbness sensation. In more advanced stage, hand muscles begin to atrophy. Many people attempt to treat CTS by surgery. However, before surgery is considered, there are several alternative treatments, including ultrasonic therapy.
Ultrasound therapy is effective at reducing the symptoms of pain, improving sensory loss, and restoring power of wrist musculature in patients with CTS [6] . A study showed that superficial continuous ultrasound reduces pain after ten treatment sessions of 5-minute duration, when compared to placebo [7]. There have been many studies conducted on the management of CTS through ultrasound therapy but there is none which directly assesses ultrasound therapy in direct comparison to other non-surgical interventions, such as splinting, oral drugs, etc [8].
On the other hand, management of CTS with manual therapy is consistently ignored as a treatment approach. Manual therapy is thought to release tissue adhesions and improve range of motion at the wrist joints. It also improves median nerve performance without any surgical intervention. Among the different manual therapy techniques, neural mobilization is a common treatment approach which has been compared to carpal bone mobilization [9]. Indeed, combined mobilization of the median nerve and carpal bones can help improve the symptoms of CTS in clinical settings [10].Rozmaryn et al. [11] have reported that nerve and tendon gliding exercises are effective in reducing pain and, hence, the chances of surgery in CTS at 23-month follow-up are consequently reduced. In contrast, other studies have failed to report any significant effects of neural mobilization exercises in the management of CTS [12][13].
To the best of our knowledge, no study has compared the effectiveness of the neural mobilization approach to ultrasound therapy approach. Thus, the aim of the present study is to compare the effectiveness of neural mobilization technique against ultrasound therapy in the management of CTS.
Methods
This was a randomized controlled trial in which 48 patients with unilateral CTS (suspected on clinical grounds and diagnosed on the basis of nerve conduction studies) were enrolled. The inclusion criteria were as follows: male and female patients between 30-50 years of age, diabetes mellitus, positive electro-diagnostic tests, acute and chronic conditions, and positive Phalen’s test. The exclusion criteria were as follows: patients with other musculoskeletal or neurological problems, neoplasms, systemic pathologies, known psycho-social problems, Herpes zoster, rheumatoid arthritis, pregnancy, hyperthyroidism, and/or known congenital abnormality of the nervous system. This study was approved by the Institutional Review Board (IRB) of Dow University of Health Sciences Karachi. It was conducted in the Physiotherapy Department of the Institute of Physical Medicine & Rehabilitation Dow University between 23rd January 2017 and 22nd July 2017. Patients were recruited from the Institute of Physical Medicine & Rehabilitation and the Rabia Moon Trust.
Patient recruitment was conducted through non-probability purposive sampling technique. After acquisition of written informed consents, patients were randomly allocated into 2 groups by simple randomization method. Group 1 (24 participants) received median nerve mobilization with gliding technique in the clinic with a home exercise program consisting of median nerve self-mobilization. Group 2 (24 participants) received ultrasound therapy on carpal tunnel with intensity of 0.8 w/cm2 for 5 minutes during each session. A total of 12 sessions were administered over a 4-week period with 3 sessions per week. Pre and post intervention data were collected from both groups using Visual Analogue Scale (VAS) to measure pain. Data were collected before the intervention and after 4 weeks of intervention. SPSS version 20 was used for data analysis; results were expressed as mean and standard deviation (SD). The initial measures from each group were compared with the final measures of the study period. Comparisons between post test results of both groups were done using paired sample t-tests, with a p-value < 0.05 considered as significant.
Results
The following is the summary of the results of the 48 patients recruited in the study who were randomly divided into two groups. The overall mean age of the patients was 40.85 years, with a standard deviation of 8.89 years. The mean age for males in our study was 41.42 years, with a standard deviation of 8.89 years; the mean age for females was 40.61 years, with SD of 9.01 years Table 1 . The assessment was done subjectively as pre and post scoring by VAS Table 2 .
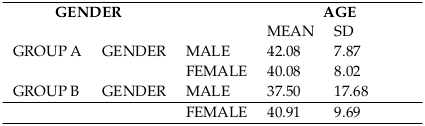

Age and gender were two demographic variables in this study. The mean age of the study population was 40.85 years with SD of 8.89. Table 1 shows the distribution (frequency and percentage) of the age of the research participants in both groups.
In group A (Neurodynamics group), out of 24 patients, 50% (12) of cases were male and 50% (12) were female. In group B (Ultrasound therapy group), out of 24 patients, 8.3% (2) of cases were male and 91.7% (22) were female. There was a significant difference in the mean rating of pain for both groups before and after treatment.
Table 2 shows that the mean pain intensity for treatment “A” (Neural Mobilization) group at baseline (pre-treatment) was 6.41 with standard deviation of 1.21; after the 4-week treatment period the pain intensity was reduced to a mean of 0.70 (SD of 0.69). The mean difference for baseline versus post intervention was found to be significant, with p-value <0.05. Similarly, the pain intensity for treatment “B” (Ultrasound Therapy) group at baseline (pre-treatment) was 7.37 with standard deviation of 0.71; after the 4-week treatment period the pain was reduced to a mean of 4.41 (SD of 1.05). Notably, the mean difference for baseline versus post intervention was also found to be significant, with p-value <0.05.
The effect of treatment A (Neurodynamics) is illustrated in Figure 1 ; it was found that the 79% (19 cases) who had moderate stage of pain and 21% (5 cases) who had severe pain all experienced successful treatment. Indeed, 100% (24) of the cases experienced only mild pain. Figure 2 illustrates that for treatment “B” (Ultrasound) group, before the treatment 54% (13) of cases had moderate pain while 46% (11) of cases had severe pain. However, after receiving intervention, 20% (5) of cases experienced mild pain and 80% (19) of cases had moderate pain.
Discussion
After twelve sessions of treatment both groups showed reduction in pre-test and post-test VAS scores of pain intensity. However, the neural mobilization group showed better results in comparison to the ultrasound therapy group. This difference between the results is attributable to the palliative effects of neural mobilization, which is supported by various studies. A randomized controlled trial conducted on tendon and nerve gliding technique, among 197 patients with CTS, showed that 70.2% of the patients who followed the nerve and tendon gliding exercises reported good or excellent results [11]. Patients of CTS have a cardinal feature of wrist pain which restricts their activities of daily living (ADLs).
Wrist pain was significantly reduced after neural gliding sessions, as supported by a study conducted in Turkey. In this study 26 patients were divided into two groups; the control group received static volar day-and-night splint while the experimental group received splint as well as neural gliding exercises for 4 weeks. Significant results were detected in both groups. However, patients who performed neural exercises experienced more rapid pain reduction and functional improvement [14]. Results in this study are supported by the fact that increase in nerve strain due to nerve bed elongation at one joint (e.g. wrist extension) is simultaneously counterbalanced by a decrease in nerve bed length at an adjacent joint (e.g. elbow flexion). Nerve gliding associated with wrist movements can be considerably increased and nerve strain substantially reduced by simultaneously moving neighboring joints [15].
Although our study shows neural gliding exercises for CTS to be more effective at reducing pain, when compared to ultrasound therapy, these findings are not in accordance with every research study conducted in CTS patients. A systematic review conducted on conservative management of CTS revealed that there is limited evidence of splinting, laser-acupuncture, yoga, and therapeutic ultrasound. Indeed, they might be effective in the short to medium term (up to 6 months). The evidence for nerve and tendon gliding exercises is even more tentative [16]. The observed contradiction from our study is probably a reflection of the paucity of evidence in the past. The present randomized controlled trial presumably fills the void of studies and may serve as a more accurate reflection on the role of neurodynamics in CTS.
With respect to the data on the ultrasonic therapy, there was a significant reduction in VAS scores both before and after treatment which has been also supported by various other studies. One study conducted in Pakistan demonstrated the effectiveness of ultrasound therapy on CTS patients by a marked difference in their VAS, Functional Status Scale and Symptom Severity Scale in the ultrasound group compared to laser therapy group [17]. Evidence suggests that ultrasound therapy when given for 15-20 min reduces the symptoms of pain, helps improve sensory loss, and provides power to the median nerve [18][19].
According to Anthony et al., ultrasound therapy is very beneficial for CTS patients and its results are long-lasting. A double blinded randomized study compared sham ultrasound treatment (for 20 sessions) in treating CTS. The results showed that there were significant improvements in the symptoms of patients at the end of the second and seventh week, and after six months [20]. In spite of regular findings of temporary improvements with ultrasound therapy, various studies have revealed that there is little evidence of ultrasound therapy in long term relief of CTS. Studies suggest only short to medium term effects of ultrasound treatment in patients with mild to moderate idiopathic CTS [21][22].
Since the findings of this study show significant improvements in both groups, we cannot disregard one intervention in favor over another intervention. Nonetheless, on the basis of the study results, neural mobilization therapy appears more effective and, thus, beneficial than ultrasound therapy in treating CTS. Employing neurodynamics may be a better course of management for coping with CTS. Future similar studies will need to be conducted with larger sample size and longer duration to further corroborate results from this present study.
Conclusion
Neural mobilization for median nerve appears more beneficial than ultrasound therapy in reducing pain intensity and functional limitations due to carpal tunnel syndrome. The results herein indicate that nerve mobilization has significant effects in reducing pain from carpal tunnel syndrome after 4 weeks of treatment sessions.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License (CC-BY 4.0) which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
List of abbreviations
ADLs: Activities of Daily Living; CTS: Carpal Tunnel Syndrome; IRB: Institutional Review Board; VAS: Visual Analogue Scale
Ethics approval and consent to participate
This study was approved by the Institutional Review Board (IRB) of Dow University of Health Sciences Karachi.
Competing interests
The authors declare that no competing interests exist.
Authors’ contributions
MA: topic selection, design, data collection and analysis, MK: topic selection, design, manuscript writing, literature search, SIA: data collection, SSH: literature search, manuscript writing. All authors read and approved the final version of manuscript.
References
-
DW
Levine,
BP
Simmons,
MJ
Koris,
LH
Daltroy,
GG
Hohl,
AH
Fossel,
JN
Katz.
A self- administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. JBJS.
1993;
75
:
1585-1592
.
View Article Google Scholar -
JN
Katz,
BP
Simmons.
Carpal tunnel syndrome. New England Journal of Medicine.
2002;
346
:
1807-1812
.
View Article Google Scholar -
I
Atroshi,
C
Gummesson,
R
Johnsson,
E
Ornstein,
J
Ranstam,
I.
Rosén.
Prevalence of carpal tunnel syndrome in a general population. Jama.
1999a;
282
:
153-158
.
-
I
Atroshi,
C
Gummesson,
R
Johnsson,
A
Sprinchorn.
Symptoms, disability, and quality of life in patients with carpal tunnel syndrome. Journal of Hand Surgery.
1999b;
24
:
398-404
.
-
KM
Ali,
BWC
Sathiyasekaran.
Computer professionals and carpal tunnel syndrome (CTS). International Journal of Occupational Safety and Ergonomics.
2006;
12
:
319-325
.
View Article Google Scholar -
GR
Ebenbichler,
KL
Resch,
P
Nicolakis,
GF
Wiesinger,
F
Uhl,
AH
Ghanem,
V
Fialka.
Ultrasound treatment for treating the carpal tunnel syndrome: randomised "sham" controlled trial. Bmj.
1998;
316
:
731-735
.
View Article Google Scholar -
O
Oztas,
B
Turan,
I
Bora,
MK
Karakaya.
Ultrasound therapy effect in carpal tunnel syndrome. Archives of physical medicine and rehabilitation.
1998;
79
:
1540-1544
.
View Article Google Scholar -
MJ
Page,
D
O'Connor,
V
Pitt,
N
Massy-Westropp.
Therapeutic ultrasound for carpal tunnel syndrome. The Cochrane Library.
2013
.
-
A
Tal-Akabi,
A
Rushton.
An investigation to compare the effectiveness of carpal bone mobilisation and neurodynamic mobilisation as methods of treatment for carpal tunnel syndrome. Manual Therapy.
2000a;
5
:
214-222
.
View Article Google Scholar -
A
Tal-Akabi,
A
Rushton.
An investigation to compare the effectiveness of carpal bone mobilisation and neurodynamic mobilisation as methods of treatment for carpal tunnel syndrome. Manual Therapy.
2000b;
5
:
214-222
.
View Article Google Scholar -
LM
Rozmaryn,
S
Dovelle,
ER
Rothman,
K
Gorman,
KM
Olvey,
JJ
Bartko.
Nerve and tendon gliding exercises and the conservative management of carpal tunnel syndrome. Journal of Hand Therapy.
1998;
11
:
171-179
.
View Article Google Scholar -
ML
Heebner,
TS
Roddey.
The effects of neural mobilization in addition to standard care in persons with carpal tunnel syndrome from a community hospital. Journal of Hand Therapy.
2008;
21
:
229-241
.
View Article Google Scholar -
E
Akalin,
Ö
El,
Ö
Peker,
Ö
Senocak,
S
Tamci,
S
Gülbahar,
R
Çakmur,
S
Öncel.
Treatment of carpal tunnel syndrome with nerve and tendon gliding exercises. American journal of physical medicine & rehabilitation.
2002;
81
:
108-113
.
View Article Google Scholar -
S
Johnson.
Carpal Tunnel Syndrome With Nerve & Tendon Gliding Exercises. 2013
.
-
MW
Coppieters,
AM
Alshami.
Longitudinal excursion and strain in the median nerve during novel nerve gliding exercises for carpal tunnel syndrome. Journal of orthopaedic Research.
2007;
25
:
972-980
.
View Article Google Scholar -
F
Goodyear-Smith,
B
Arroll.
What can family physicians offer patients with carpal tunnel syndrome other than surgery? A systematic review of nonsurgical management. The Annals of Family Medicine.
2004;
2
:
267-273
.
View Article Google Scholar -
FU
Saeed,
S
Hanif,
M
Aasim.
The effects of laser and ultrasound therapy on carpal tunnel syndrome. Pakistan J Med Heal Sci.
2012;
6
:
238-241
.
-
D
O'Connor,
SC
Marshall,
N
Massy-Westropp,
V
Pitt.
Non-surgical treatment (other than steroid injection) for carpal tunnel syndrome. The Cochrane Library.
2003
.
-
M
Muller,
D
Tsui,
R
Schnurr,
L
Biddulph-Deisroth,
J
Hard,
JC
MacDermid.
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome: a systematic review. Journal of Hand Therapy.
2004;
17
:
210-228
.
View Article Google Scholar -
AJ
Viera.
Management of carpal tunnel syndrome. Am Fam Physician.
2003;
68
:
265-72
.
PubMed Google Scholar -
GR
Ebenbichler,
KL
Resch,
P
Nicolakis,
GF
Wiesinger,
F
Uhl,
AH
Ghanem,
V
Fialka.
Ultrasound treatment for treating the carpal tunnel syndrome: randomised "sham" controlled trial. Bmj.
1998;
316
:
731-735
.
View Article Google Scholar -
AA
Gerritsen,
MC
de Krom,
MA
Struijs,
RJ
Scholten,
HC
de Vet,
LM
Bouter.
Conservative treatment options for carpal tunnel syndrome: a systematic review of randomised controlled trials. Journal of neurology.
2002;
249
:
272-280
.
View Article Google Scholar
Comments
Downloads
Article Details
Volume & Issue : Vol 5 No 4 (2018)
Page No.: 2187-2193
Published on: 2018-04-23
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 17024 times
- Download PDF downloaded - 4449 times
- View Article downloaded - 0 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}