

Copyrights: Phuong Thu Vu Hoang, Quang An Lam, Minh Xuan Ngo, Anh Thu Ha Nguyen, Chung Thuy Tran Phan, 2023. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Introduction: The most common sensory disorder, hearing loss, may result from genetic causes. Various inheritance patterns exist, such as X-linked, autosomal dominant, autosomal recessive, and mitochondrial. However, the genetic underpinnings of racial distinctiveness and regional variation were incompletely understood. To fully evaluate the ethnic specificity of gap junction protein beta 2 (GJB2) and tectorin alpha (TECTA) mutations in this region, data from all GJB2 and TECTA gene studies on Asian children with hearing impairment were pooled and used in this research.
Methods: All nonsyndromic hearing loss studies on the prevalence of GJB2 or TECTA mutations published between 1990 and 2022 were retrieved from the PubMed database, evaluated for risk of bias, and meta-analyzed.
Results: Twelve studies were chosen, representing twelve prevalence estimates. The prevalence of GJB2 and TECTA mutations in Asian patients with nonsyndromic hearing loss was 13.36% (95% confidence interval [CI]: 7.74%?20.14%), varying significantly among trials (I2 = 96.74%; P < 0.001). The pooled prevalence of TECTA and GJB2 mutations was 3.6% (95% CI: 1.9%? 5.7%) and 24.06% (95% CI: 11.43%?31.35%), respectively.
Conclusions: There was an association between TECTA/GJB2 mutations and hearing impairment, but there were also regional and ethnic differences in mutation prevalence. Studies with larger sample sizes and genetic analyses based on long-read sequencing are needed to understand the mutations resulting in hearing loss.
Introduction
The ear loses its ability to change sound’s mechanical energy into electrical energy, leading to hearing loss. The cochlea’s hair cells maintain this role by converting oscillation into neuronal impulses and sending messages to the brain’s cortex via the VIII nerve1. Conductive hearing loss results from a disruption of sound transmission at the outer and/or middle ear. In contrast, sensorineural hearing loss (SNHI) occurs when the inner ear cannot communicate with the brain. Hearing loss can be genetic and/or acquired, depending on when it first appears2, 3. One in 1000 newborns has a hearing impairment, the most frequent sensory disorder. The most prevalent sensory disorder is believed to be of genetic origin, accounting for roughly 50% of all cases4.
Hearing loss is caused by gene mutations in 50% of cases. Environmental factors such as ototoxic medications, prematurity, and cranial trauma account for the remaining 50%. Approximately 70% of cases of inherited hearing loss are attributed to nonsyndromic hearing loss. Nonsyndromic genetic deafness has various inheritance patterns, such as autosomal recessive and dominant, X-linked, and mitochondrial2. Autosomal recessive inheritance, due to mutations in the gap junction protein beta 2 (GJB2) gene, is more common (80%) than autosomal dominant (AD) inheritance (20%) in severe and congenital pre-lingual deafness5. AD nonsyndromic hearing loss (ADNSHL) is a condition with diverse genetic and clinical features. Tectorin alpha (TECTA) mutations have been identified as contributing to ADNSHL in diverse populations, differing in their ages of onset and degrees of auditory impairment, rates of advancement, and extent of participation6, 7, 8. The association between deafness and TECTA mutations is the subject of an ongoing debate regarding the underlying mechanisms. Some studies have identified missense mutations in its zona pellucida domain as a potential biological factor contributing to ADSHNL.
These studies considered only parts of genetic figures related to ethnic particularity and regional differences. Due to the small sample sizes of case-control studies, detecting minor genetic associations in humans was difficult. To learn more about this variable, we need a meta-analysis of the association between ethnic specificity and mutations in GJB2 and TECTA. In this study, all published studies on the GJB2 and TECTA genes in Asian pediatric populations with hearing impairment were used in a combined meta-analysis. Based on the evaluation of the relationship between GJB2 and TECTA mutations and hearing impairment and the genetic heterogeneity effect, a stratified meta-analysis was performed to determine whether GJB2 and TECTA mutations causing hearing loss in Asian children are specific to that ethnic group.
Methods
Eligibility requirements
All nonsyndromic hearing loss studies published since 1990 were considered for inclusion if the prevalence of GJB2 or TECTA mutations was reported or could be calculated from the available data. Studies that presented assumptions based on specific subgroups of the overall population were excluded (e.g., women or related family). Notably, certain populations, such as the Han Chinese population or those participating in the hospital-based studies, were not excluded since they were considered to reflect the broader population within a given geographic region.
Search strategy
Using a search methodology that combined appropriate key phrases and subject-specific terms within the respective databases, PubMed was searched through November 6, 2022. The search strategy incorporated GJB2 (235delC and V37I) or TECTA-related terms with study design-related terms, such as epidemiology, cohort, cross-sectional, and observational study.
The titles of the identified articles were examined, and those that were irrelevant to this study were eliminated. After checking the abstracts, the full texts of the remained articles were examined to identify pertinent investigations that satisfied the established inclusion criteria.
Additional pertinent articles were identified by reviewing the reference lists of full-text articles.
Risk of bias assessment
The potential bias in the included studies was assessed using the Agency for Healthcare Research and Quality (AHRQ) checklist, which is intended specifically for cross-sectional or prevalence studies9. This evaluation was conducted independently. The methodology checklist developed by the AHRQ comprises eleven parts. A score of “1” is assigned to each item if the response is affirmative, while a score of “0” is assigned for an unclear or negative response. Research investigations are classified into three categories of bias risk based on their quality scores: 0–3, high; 4–7, moderate; 8–11, low. The AHRQ methodology checklist findings were subjected to cross-validation, and any discrepancies were resolved through team deliberation.
Data extraction
The data extraction from each article was standardized using a data collection form. The extracted data included information on the sampled population, prevalence rate, period of the estimated prevalence (such as a point or a year), and any reported rates stratified by specific GJB2 or TECTA variants, age, sex, or location. The form also contained sections to gather relevant information to assess potential bias.
Analysis
The average carrier frequency of the 235delC and p.V37I mutations of the GJB2 and TECTA genes was determined in each study. According to the distribution of carriers, the included populations were divided into two categories: patients with nonsyndromic hearing loss with TECTA or GJB2 gene mutations.
The investigations were subjected to preliminary descriptive statistics. The diversity among assumptions was evaluated using the I2 statistic, which represents the proportion of variation across studies that was not due to sampling error. An I2 >75% indicates considerable heterogeneity. A model with random effects was used to conduct a meta-analysis. A pooled prevalence with a 95% confidence interval (CI) was calculated. The statistical analyses were performed using STATA software (version 14).

| ID | References | Survey period | Sample size (n) | Country | Sex (F/M) | Mean age (± SD/range) |
|---|---|---|---|---|---|---|
| 1 | Identification of novel variants in Iranian consanguineous pedigrees with nonsyndromic hearing loss by next-generation sequencing 10 | 2020 | 44 | Iran | NA | 39.6 (7–60) |
| 2 | The prevalence and clinical characteristics of TECTA-associated autosomal dominant hearing loss 11 | 2000–2017 | 812 | Japan | NA | 37.1 (0–86) |
| 3 | Mutation analysis of common GJB2, SCL26A4 and 12S rRNA genes among 380 deafness patients in northern China 12 | NA | 380 | China | 199/181 | 9.9 (0.5–38) |
| 4 | Targeted next-generation sequencing successfully detects causative genes in Chinese patients with hereditary hearing loss 13 | NA | 116 | China | 56/60 | 0–70 |
| 5 | The prevalence of the 235delC GJB2 mutation in a Chinese deaf population 14 | NA | 3004 | China | 1298/1706 | 13.8 (±4.5) |
| 6 | TECTA mutations in Japanese with mid-frequency hearing loss affected by zona pellucida domain protein secretion 15 | NA | 139 | Japan | NA | NA |
| 7 | Prevalence of p.V37I variant of GJB2 in mild or moderate hearing loss in a pediatric population and the interpretation of its pathogenicity 16 | 2010–2012 | 380 | Korea | NA | NA |
| 8 | High prevalence of V37I genetic variant in the connexin-26 (GJB2) gene among nonsyndromic hearing-impaired and control Thai individuals 17 | 2000–2002 | 166 | Thailand | 89/77 | NA |
| 9 | GJB2 (connexin 26) mutations and childhood deafness in Thailand 18 | NA | 17 | Thailand | 10/7 | NA |
| 10 | Genetic etiology study of the nonsyndromic deafness in Chinese Hans by targeted next-generation sequencing 19 | NA | 190 | China | 53/84 | 14 (0–50) |
| 11 | First molecular screening of deafness in the Altai Republic population 20 | NA | 76 | Altai Republic | 39/37 | 30.2 (3–80) |
| 12 | The p.V37I exclusive genotype of GJB2: A genetic risk-indicator of postnatal permanent childhood hearing impairment 21 | 2009–2010 | 45 | China | NA | 7 (3.9–10.1) |
| ID | Author | Publication year | Gene | Gene subgroup | Sample (n) | No. of cases (n) | Quality rating | ||
|---|---|---|---|---|---|---|---|---|---|
| 1 | Fatemeh Bitarafan | 2020 | TECTA | 44 | 26 | Moderate | |||
| 2 | Rika Yasukawa | 2019 | TECTA | 812 | 76 | Moderate | |||
| 3 | Jing Pan | 2017 | GJB2 | 235delC | 380 | 9 | Moderate | ||
| 4 | Siqi Chen | 2016 | TECTA | 116 | 9 | Moderate | |||
| GJB2 | 116 | 37 | Moderate | ||||||
| 5 | Pu Dai | 2007 | GJB2 | 235delC | 3004 | 488 | Moderate | ||
| 6 | Hideaki Moteki | 2012 | TECTA | 139 | 4 | High | |||
| 7 | So Young Kim | 2013 | GJB2 | p.V37I | 380 | 4 | Low | ||
| 8 | Duangrurdee Wattanasirichaigoon | 2004 | GJB2 | p.V37I | 166 | 56 | Moderate | ||
| 9 | T Kudo | 2001 | GJB2 | 17 | 4 | High | |||
| 10 | Tao Yang | 2013 | GJB2 | 190 | 36 | High | |||
| 11 | Olga Posukh | 2005 | GJB2 | 76 | 18 | High | |||
| 12 | Lei Li | 2012 | GJB2 | p.V37I | 45 | 9 | Moderate | ||



Results
Search results
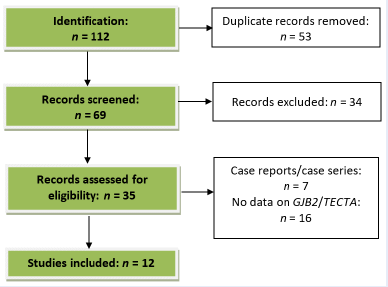
The PubMed database search identified 112 publications, of which 69 were chosen for full-text review. Their reference lists led to the identification of 12 additional studies. The screening procedure is illustrated in Figure 1.
After a full-text evaluation, 23 articles were excluded. Therefore, 12 studies were selected for review (Table 1), representing 12 prevalence approximations. Most of the 12 studies were conducted in Asia within the past two decades. Five of the 12 studies were performed in China, two in Thailand, and two in Japan. They included sample sizes from 17 to 3004.
Risk of bias
Table 2 provides a concise overview of the bias risk associated with the articles included in this study. None of the studies met all of the checklist’s quality evaluation criteria. The AHRQ scores for included articles varied from two to eight. Most studies (7/12) met at least 50% of the quality evaluation criteria. One study (8.3%; Hideaki Moteki et al.)15 was deemed to have a low risk of bias for the participants and assessment of the outcomes, while four (33.3%) were deemed to have a substantial risk of bias.
Prevalence rates were often presented in an article or calculatable from the provided data. Iran had the highest prevalence of TECTA mutations (Fatemeh Bitarafan, 2020)10, while Japan had the lowest prevalence (Hideaki Moteki, 2012)15. Thailand had the highest prevalence of GJB2 mutations (Duangrurdee Wattanasirichaigoon, 2002)17, while Korea had the lowest prevalence (So Young Kim, 2013)16.
Meta-analysis
This study investigated the prevalence of GJB2/TECTA mutations in individuals with nonsyndromic hearing loss in Asia. Its findings indicate that the frequency of GJB2/TECTA mutations in Asian individuals with nonsyndromic hearing loss was 13.36% (95% CI: 7.74%–20.14%). The included studies showed significant heterogeneity, with an I2 of 96.74% (P < 0.001; Figure 2, Figure 3). An asymmetric funnel plot suggested the possibility of publication bias.
A funnel plot was used to determine whether there was any publication bias in the included articles. Based on the study distribution (Figure 3), the funnel plot is almost the same on both sides. The meta-analysis conducted did not show any notable indication of publication bias based on the included studies.
Four studies examined the number of people with nonsyndromic hearing loss with a TECTA mutation. The combined occurrence rate of TECTA mutations was 3.6% (95% CI: 1.9%–5.8%). The studies exhibited moderate heterogeneity (I2 = 37.87%, P = 0.18).
Four studies reported the occurrence of GJB2 mutations in individuals with nonsyndromic hearing loss. The combined prevalence of GJB2 mutations was 24.06% (95% CI: 11.43–31.36). The studies exhibited moderate heterogeneity (I2 = 53.6%, P = 0.09).
Two studies reported the prevalence of the GJB2 gene variant 235delC in individuals with nonsyndromic hearing loss. Its pooled frequency was 16.6% (95% CI: 15.4%–17.9%).
Three studies explored the number of people with nonsyndromic hearing loss with the GJB2 gene variant p.V37I. Its pooled frequency was 14.7% (95% CI: 0%–48.6%).
Discussion
The commonly observed inherited etiology of SNHI is attributed to recessive variants in the GJB2 gene. The prevalence of GJB2 mutations varies significantly among different ethnic communities. For example, Europeans carry c.35delG (p.Gly12ValfsTer2) and c.101T>C (p.Met34Thr) mutations22, 23, 24, while East Asians carry c.235delC (p.Leu79CysfsTer3) and c.109G>A (p.Val37Ile) mutations14, 25, 26, 27. Additionally, Ghanaians carry the c.427C>T (p.Arg143Trp) mutation28. Three plausible mechanisms that could account for these inconclusive results exist. SNHI could also be caused by pathogenic mutations in other genes known to cause deafness. In such cases, patients who do not present with the confirmatory symptoms for SNHI may still carry mono-allelic GJB2 variants as incidental carriers. Furthermore, mutation frequencies fluctuate widely between countries.
One study on ADNSHL communities in Japan found a prevalence of TECTA mutations of 2.9% (4/139), with an incidence of 7.7% (4/52) in those with moderate hearing loss15. These findings indicate that the frequency of TECTA mutations in the Japanese is relatively low compared to Iranians, whose prevalence was >50%10. The prevalence of GJB2 mutations can vary widely even within the same country. In 2017, Jing Pan reported a prevalence of 2.4% for GJB2 mutations in Northern China, while Pu Dai reported a prevalence of 16.2% in Chinese patients29, 30. Despite having a pooled prevalence of 3.6% (95% CI: 1.9%–5.7%) for TECTA mutations and 24.06% (95% CI: 11.43%–31.35%) for GJB2 mutations, this comparison indicates geographical differences in mutation frequency, emphasizing the need for further research on regional risk factors such as lifestyles, education, and life qualities.
The prevalence of each mutation shows variation across different ethnic groups and countries. The 35delG mutation has been observed in up to 85% of Caucasians31. In contrast, the 235delC mutation has been identified most frequently in the Chinese32 (20.3%), Koreans33 (6.9%), and Japanese34 (49.8%). The c.167delT mutation has been found in 4.03% of Ashkenazi Jews35 and 2% of Argentianians36. These results indicate ethnic differences in mutation prevalence, emphasizing the need for further studies with larger sample sizes and genetic analyses based on long-read sequencing to better understand mutations associated with hearing impairment.
This study’s main limitation was the heterogeneity of its included studies. The population of individuals suspected of hearing loss varied across studies, and most were not precisely defined. Several studies focused exclusively on children, while most did not provide any particular age range. The allele frequencies in various countries may be influenced by particular population samples, resulting in sampling bias. In addition, the ethnic or racial origin of part of the study population was not specified, and the scope of this analysis was limited to the geographic aspect and did not encompass ethnicity. Another limitation of this study was that its data was only extracted from the Pubmed database. Therefore, some studies indexed in Embase, Web of Science, or Scopus were not included.
Conclusions
Our results showed an association between TECTA/GJB2 mutations and hearing impairment, but there were also regional and ethnic differences in mutation prevalence. However, studies with larger sample sizes and genetic analyses based on long-read sequencing are needed to better understand the changes resulting in hearing loss.
Abbreviations
AD: autosomal dominant; AHRQ: Agency for Healthcare Research and Quality; GJB2: gap junction protein beta 2; SNHL: sensorineural hearing loss; TECTA: tectorin alpha
Acknowledgments
We sincerely thank PhD. MD Quang Minh Le Tran (Director of Ear Nose Throat Hospital Hochiminh City) for the permission to perform the research.
Author’s contributions
Minh Xuan Ngo and Chung Thuy Tran Phan conceived of the presented idea, developed the theory and supervised the findings of this study. Phuong Hoang Vu, Anh Thu Ha Nguyen and Thanh Vu Nguyen worked out the technical details, and performed the numerical calculations for the suggested experiment, verified the numerical results of the study. Phuong Hoang Vu and Quang An Lan interpreted the results and worked on the manuscript. All authors read and approved the final version of manuscript.
Funding
This study is supported by a grant from Vietnam National University Ho Chi Minh City (VNU-HCM) with grant number GENE2020-44-01.
Availability of data and materials
Data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
-
Alberti
P.W.,
The anatomy and physiology of the ear and hearing. Occupational exposure to noise: evaluation, prevention and controlWorld Health Organisation 2001.
Google Scholar -
Tekin
M.,
Arnos
K.S.,
Pandya
A.,
Advances in hereditary deafness. Lancet.
2001;
358
(9287)
:
1082-90
.
View Article PubMed Google Scholar -
Smith
R.J.,
Bale
J.F.,
White
K.R.,
Sensorineural hearing loss in children. Lancet.
2005;
365
(9462)
:
879-90
.
View Article PubMed Google Scholar -
Gorlin
R.J.,
Cohen
M.M.,
Epimeiology, Etiology and Genetic Patterns. Hereditary hearing loss and its syndromesOxford University Press: USA; 1995.
Google Scholar -
Kral
A.,
O'Donoghue
G.M.,
Profound deafness in childhood. The New England Journal of Medicine.
2010;
363
(15)
:
1438-50
.
View Article PubMed Google Scholar -
Hereditary hearing loss homepage. http://hereditaryhearingloss.org..
.
-
Hutchin
T.,
Coy
N.N.,
Conlon
H.,
Telford
E.,
Bromelow
K.,
Blaydon
D.,
Assessment of the genetic causes of recessive childhood non-syndromic deafness in the UK - implications for genetic testing. Clinical Genetics.
2005;
68
(6)
:
506-12
.
View Article PubMed Google Scholar -
Shearer
A.E.,
DeLuca
A.P.,
Hildebrand
M.S.,
Taylor
K.R.,
Gurrola
J.,
Scherer
S.,
Comprehensive genetic testing for hereditary hearing loss using massively parallel sequencing. Proceedings of the National Academy of Sciences of the United States of America.
2010;
107
(49)
:
21104-9
.
View Article PubMed Google Scholar -
Rostom
A.,
Dubé
C.,
Cranney
A.,
Celiac Disease. Rockville (MD): Agency for Healthcare Research and Quality (US); 2004 Sep. (Evidence Reports/Technology Assessments, No. 104.) Appendix D. Quality Assessment Forms. 2004. https://www.ncbi.nlm.nih.gov/books/NBK35156/. 2004
.
-
Dai
P.,
Yu
F.,
Han
B.,
Yuan
Y.,
Li
Q.,
Wang
G.,
The prevalence of the 235delC GJB2 mutation in a Chinese deaf population. Genetics in Medicine.
2007;
9
(5)
:
283-9
.
View Article PubMed Google Scholar -
Moteki
H.,
Nishio
S.Y.,
Hashimoto
S.,
Takumi
Y.,
Iwasaki
S.,
Takeichi
N.,
TECTA mutations in Japanese with mid-frequency hearing loss affected by zona pellucida domain protein secretion. Journal of Human Genetics.
2012;
57
(9)
:
587-92
.
View Article PubMed Google Scholar -
Kim
S.Y.,
Park
G.,
Han
K.H.,
Kim
A.,
Koo
J.W.,
Chang
S.O.,
Prevalence of p.V37I variant of GJB2 in mild or moderate hearing loss in a pediatric population and the interpretation of its pathogenicity. PLoS One.
2013;
8
(4)
:
e61592
.
View Article PubMed Google Scholar -
Wattanasirichaigoon
D.,
Limwongse
C.,
Jariengprasert
C.,
Yenchitsomanus
P.T.,
Tocharoenthanaphol
C.,
Thongnoppakhun
W.,
High prevalence of V37I genetic variant in the connexin-26 (GJB2) gene among non-syndromic hearing-impaired and control Thai individuals. Clinical Genetics.
2004;
66
(5)
:
452-60
.
View Article PubMed Google Scholar -
Kudo
T.,
Ikeda
K.,
Oshima
T.,
Kure
S.,
Tammasaeng
M.,
Prasansuk
S.,
GJB2 (connexin 26) mutations and childhood deafness in Thailand. Otology & Neurotology.
2001;
22
(6)
:
858-61
.
View Article PubMed Google Scholar -
Yang
T.,
Wei
X.,
Chai
Y.,
Li
L.,
Wu
H.,
Genetic etiology study of the non-syndromic deafness in Chinese Hans by targeted next-generation sequencing. Orphanet Journal of Rare Diseases.
2013;
8
(1)
:
85
.
View Article PubMed Google Scholar -
Posukh
O.,
Pallares-Ruiz
N.,
Tadinova
V.,
Osipova
L.,
Claustres
M.,
Roux
A.F.,
First molecular screening of deafness in the Altai Republic population. BMC Medical Genetics.
2005;
6
(1)
:
12
.
View Article PubMed Google Scholar -
Li
L.,
Lu
J.,
Tao
Z.,
Huang
Q.,
Chai
Y.,
Li
X.,
The p.V37I exclusive genotype of GJB2: a genetic risk-indicator of postnatal permanent childhood hearing impairment. PLoS One.
2012;
7
(5)
:
e36621
.
View Article PubMed Google Scholar -
Bitarafan
F.,
Seyedena
S.Y.,
Mahmoudi
M.,
Garshasbi
M.,
Identification of novel variants in Iranian consanguineous pedigrees with nonsyndromic hearing loss by next-generation sequencing. Journal of Clinical Laboratory Analysis.
2020;
34
(12)
:
e23544
.
View Article PubMed Google Scholar -
Yasukawa
R.,
Moteki
H.,
Nishio
S.Y.,
Ishikawa
K.,
Abe
S.,
Honkura
Y.,
The Prevalence and Clinical Characteristics of TECTA-Associated Autosomal Dominant Hearing Loss. Genes.
2019;
10
(10)
:
744
.
View Article PubMed Google Scholar -
Pan
J.,
Xu
P.,
Tang
W.,
Cui
Z.,
Feng
M.,
Wang
C.,
Mutation analysis of common GJB2, SCL26A4 and 12S rRNA genes among 380 deafness patients in northern China. International Journal of Pediatric Otorhinolaryngology.
2017;
98
:
39-42
.
View Article PubMed Google Scholar -
Chen
S.,
Dong
C.,
Wang
Q.,
Zhong
Z.,
Qi
Y.,
Ke
X.,
Targeted Next-Generation Sequencing Successfully Detects Causative Genes in Chinese Patients with Hereditary Hearing Loss. Genetic Testing and Molecular Biomarkers.
2016;
20
(11)
:
660-5
.
View Article PubMed Google Scholar -
Pollak
A.,
Skórka
A.,
Mueller-Malesińska
M.,
Kostrzewa
G.,
Kisiel
B.,
Waligóra
J.,
M34T and V37I mutations in GJB2 associated hearing impairment: evidence for pathogenicity and reduced penetrance. American Journal of Medical Genetics. Part A.
2007;
143A
(21)
:
2534-43
.
View Article PubMed Google Scholar -
Chan
D.K.,
Schrijver
I.,
Chang
K.W.,
Connexin-26-associated deafness: phenotypic variability and progression of hearing loss. Genetics in Medicine.
2010;
12
(3)
:
174-81
.
View Article PubMed Google Scholar -
Gasparini
P.,
Rabionet
R.,
Barbujani
G.,
Melçhionda
S.,
Petersen
M.,
Br∅ndum-Nielsen
K.,
High carrier frequency of the 35delG deafness mutation in European populations. Genetic Analysis Consortium of GJB2 35delG. European Journal of Human Genetics.
2000;
8
(1)
:
19-23
.
View Article PubMed Google Scholar -
Hwa
H.L.,
Ko
T.M.,
Hsu
C.J.,
Huang
C.H.,
Chiang
Y.L.,
Oong
J.L.,
Mutation spectrum of the connexin 26 (GJB2) gene in Taiwanese patients with prelingual deafness. Genetics in Medicine.
2003;
5
(3)
:
161-5
.
View Article PubMed Google Scholar -
Oguchi
T.,
Ohtsuka
A.,
Hashimoto
S.,
Oshima
A.,
Abe
S.,
Kobayashi
Y.,
Clinical features of patients with GJB2 (connexin 26) mutations: severity of hearing loss is correlated with genotypes and protein expression patterns. Journal of Human Genetics.
2005;
50
(2)
:
76-83
.
View Article PubMed Google Scholar -
Han
S.H.,
Park
H.J.,
Kang
E.J.,
Ryu
J.S.,
Lee
A.,
Yang
Y.H.,
Carrier frequency of GJB2 (connexin-26) mutations causing inherited deafness in the Korean population. Journal of Human Genetics.
2008;
53
(11-12)
:
1022-8
.
View Article PubMed Google Scholar -
Brobby
G.W.,
Müller-Myhsok
B.,
Horstmann
R.D.,
Connexin 26 R143W mutation associated with recessive nonsyndromic sensorineural deafness in Africa. The New England Journal of Medicine.
1998;
338
(8)
:
548-50
.
View Article PubMed Google Scholar -
Azaiez
H.,
Chamberlin
G.P.,
Fischer
S.M.,
Welp
C.L.,
Prasad
S.D.,
Taggart
R.T.,
GJB2: the spectrum of deafness-causing allele variants and their phenotype. Human Mutation.
2004;
24
(4)
:
305-11
.
View Article PubMed Google Scholar -
Matos
T.D.,
Caria
H.,
Simões-Teixeira
H.,
Aasen
T.,
Nickel
R.,
Jagger
D.J.,
A novel hearing-loss-related mutation occurring in the GJB2 basal promoter. Journal of Medical Genetics.
2007;
44
(11)
:
721-5
.
View Article PubMed Google Scholar -
Estivill
X.,
Fortina
P.,
Surrey
S.,
Rabionet
R.,
Melchionda
S.,
D'Agruma
L.,
Connexin-26 mutations in sporadic and inherited sensorineural deafness. Lancet.
1998;
351
(9100)
:
394-8
.
View Article PubMed Google Scholar -
Liu
X.Z.,
Xia
X.J.,
Ke
X.M.,
Ouyang
X.M.,
Du
L.L.,
Liu
Y.H.,
The prevalence of connexin 26 ( GJB2) mutations in the Chinese population. Human Genetics.
2002;
111
(4-5)
:
394-7
.
View Article PubMed Google Scholar -
Lee
K.Y.,
Choi
S.Y.,
Bae
J.W.,
Kim
S.,
Chung
K.W.,
Drayna
D.,
Molecular analysis of the GJB2, GJB6 and SLC26A4 genes in Korean deafness patients. International Journal of Pediatric Otorhinolaryngology.
2008;
72
(9)
:
1301-9
.
View Article PubMed Google Scholar -
Tsukada
K.,
Nishio
S.,
Usami
S.,
Consortium
undefined Deafness Gene Study,
A large cohort study of GJB2 mutations in Japanese hearing loss patients. Clinical Genetics.
2010;
78
(5)
:
464-70
.
View Article PubMed Google Scholar -
Morell
R.J.,
Kim
H.J.,
Hood
L.J.,
Goforth
L.,
Friderici
K.,
Fisher
R.,
Mutations in the connexin 26 gene (GJB2) among Ashkenazi Jews with nonsyndromic recessive deafness. The New England Journal of Medicine.
1998;
339
(21)
:
1500-5
.
View Article PubMed Google Scholar -
Dalamón
V.,
Wernert
M. Florencia,
Lotersztein
V.,
Craig
P.O.,
Diamante
R.R.,
Barteik
M.E.,
Identification of four novel connexin 26 mutations in non-syndromic deaf patients: genotype-phenotype analysis in moderate cases. Molecular Biology Reports.
2013;
40
(12)
:
6945-55
.
View Article PubMed Google Scholar
Comments
Article Details
Volume & Issue : Vol 10 No 6 (2023)
Page No.: 5717-5725
Published on: 2023-06-30
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 4148 times
- PDF downloaded - 1508 times
- XML downloaded - 130 times
