

Copyrights: Le Phuong Mai, Vo Ngoc Anh Tho, Duong Thi Thanh Van, Truong Thien Phu, 2024. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: Keratitis caused by Nocardia, a Gram-positive bacterium prevalent in soil, is an infrequent ocular infection typically following corneal trauma or exposure to soil or vegetation. Nocardia farcinica, in particular, is an exceedingly rare causative agent of keratitis, with few documented cases worldwide and none previously reported in Vietnam.
Case Presentation: We report the first documented case of N. farcinica keratitis in Viet Nam, presenting as a corneal abscess in a 70- year-old male farmer following phacoemulsification surgery. Despite prolonged treatment with corticosteroids and atropine eye drops, the patient experienced persistent pain, tearing, and poor vision improvement. A definitive diagnosis was achieved through the culture of corneal swabs on blood agar medium, which yielded dry, wrinkled yellow colonies identified as Nocardia spp., with subsequent MALDI-TOF MS (VITEK-MS) confirmation of N. farcinica. The patient showed significant improvement following treatment with 0.3% tobramycin.
Conclusion: This case underscores the importance of considering N. farcinica in the differential diagnosis of post-surgical keratitis, particularly in patients unresponsive to standard treatments. It highlights the necessity of a thorough medical history, clinical examination, and the pivotal role of microbiological culture and molecular identification techniques in diagnosing rare infectious agents. This case adds to the global repository of Nocardia keratitis cases and suggests a need for awareness and diagnostic readiness for such infections, especially in rural farming communities.
Introduction
Nocardia is a rare agent of infectious keratitis, accounting for only about 3% of cases1, 2, but it can be misdiagnosed as a fungal or viral infection, thus limiting the treatment and leading to vision damage. Nocardia keratitis has been reported only in case reports and a few case series, often occurring after trauma or surgery, including phacoemulsification (PHACO) surgery, and Nocardia asteroides is the most common causative pathogen2, 3. Nocardia farcinica was first described by Edmond Nocard in 1888 as causing lung infections and brain abscesses4. In 1997, Eggink et al. first reported a case of keratitis caused by N. farcinica in a patient who used contact lenses that were improperly cleaned with water from the sink5, and to date, there have been few reports of keratitis caused by this bacteria and none in Vietnam. Here, we describe a case of corneal abscess caused by N. farcinica after phacoemulsification surgery.
Case report
A 70-year-old male patient, working as a farmer, with no medical history recorded, was treated at Cho Ray Hospital in November 2023. The patient presented with symptoms of right eye pain, tearing, and vision that did not improve after surgery. About two months before admission, the patient had PHACO surgery at Phu Yen Hospital. After surgery, the patient immediately returned to farming. About one week later, symptoms of increasing eye pain, tearing, and stinging appeared and vision after surgery did not improve. The patient was treated with corticosteroid drops (Pred Forte) with a diagnosis of uveitis after PHACO surgery at the outpatient department of Eye hospital. After one week of treatment, the patient was given diagnostic tests for hepatitis B and C, syphilis, and HIV and a chest X-ray prior to long-term corticosteroid treatment. Diagnostic tests were negative but chest X-ray results showed damage to the lung apex, so the patient was transferred to a tuberculosis specialist hospital where they were diagnosed with AFB-negative pulmonary tuberculosis and treated with anti-tuberculosis drugs (Turbezid 600 mg/day and ethambutol 600 mg/day). During tuberculosis treatment, the patient continued to use Pred Forte eyedrops. Eye symptoms decreased but the discharge remained and vision did not improve. He was admitted to Cho Ray Hospital and discontinued Pred Forte after admission (total duration of Pred Forte was two months).
Clinical symptoms at admission included the following: visual acuity of the right eye to distinguish between light and dark; intense eye pressure; conjunctival hyperemia; corneal edema; central corneal abscess near the main incision, size about 4.0 x 5.0 mm; anterior chamber had fibrin sticking from the back of the cornea to the pupillary area; the anterior chamber pus was 1.5 mm; the posterior structures were difficult to observe. Diagnosis at the time of admission: right eye corneal abscess after PHACO surgery; tuberculosis under treatment. The patient had corneal fluid samples taken for gram staining, fungal screening, and culture before treatment. After taking the specimen, the patient was given oral medications: levofloxacin (500 mg/day), itraconazole (200 mg/day), acetazolamide (500 mg/day), kalium (500 mg/day) and Azarga eyedrops (every 12 hours), Natacin (every 2 hours), Vigamox (every 2 hours), and atropine (every 2 hours). On the fifth day after admission, the patient still had the following symptoms: eye pain at night; right eye corneal edema; ulcer at the edge of the edge at the 9 o'clock position with a feathered edge; ulcer with mucous surface, size 4.0 x 5.0 mm, monitored for corneal perforation; anterior chamber present but irregular, shallow towards the temple; pupil distorted towards the temple; ciliary body reaction 3+.


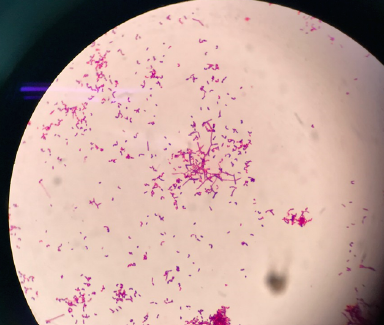
Gram stain results did not find bacteria or fungi. However, on the fifth day, dry, yellow wrinkled, colonies appeared on the blood agar, denting the agar. On the colony’s Gram stain, bacteria appeared thin, filamentous, branching, and irregular, which suggested Nocardia. The MALDI-TOF MS (matrix-assisted laser desorption ionization-time of flight mass spectrometry) method using the VITEK-MS system (bioMérieux SA, Marcy-l'Étoile, France) identified the bacteria as Nocardia farcinica.
After obtaining the bacterial culture results, the patient was stopped with levofloxacin antibiotics, supplemented with intravenous antibiotics (imipenem 500 mg every 6 hours), oral antibiotics trimethoprim/sulfamethoxazole (960 mg every 12 hours) and Azarga eyedrops (every 12 hours), Natacin (every 2 hours), Vigamox (every 2 hours), and atropine (every 2 hours). A second corneal smear sample was taken for staining, bacterial culture, and molecular biology testing for tuberculosis bacteria. The results of the culture and tuberculosis test were negative. On the 10th day after admission, the patient's right eye had reduced pain, and examination results showed reduced anterior chamber fibrin, reduced anterior chamber pus streaks, corneal edema, thinning of the abscess, and average eye pressure.
Discussion
Nocardia farcinica belongs to the genus Nocardia, which are filamentous, aerobic, weakly acid-resistant Gram-positive bacilli that commonly live in environments such as soil, water, mud, dust, and decomposing plants. The genus Nocardia has about 87 species, of which the most common is N. asteroides. Other less common species such as N. farcinica, N. brasiliensis, N. cyriacigeorgica, and N. exalbida often cause lung infections in immunocompromised patients and can spread to other organs via the bloodstream, but can also cause infection in immunocompetent patients whose wounds are exposed to environments containing bacteria6. Although ocular infections caused by Nocardia are rare1, they are an important cause of corneal infections7. Research on cases of Nocardia infections in China (2009–2021) shows that the rate of eye infections caused by this bacteria is only 2% (9/441 patients) and the majority of patients are over 45 years old8. In Italy, studies from 2000 to 2022 showed that Nocardia-related eye infections accounted for 1% of cases, mainly due to N. asteroides9. Very few cases have been reported of ocular infections due to N. farcinica.
Nocardia farcinica was first described by Edmond Nocard in 18884, and subsequent reports showed that the bacterium often causes lung infections and brain abscesses and can cause disseminated Nocardiosis (Nocardiosis), especially in immunodeficient patients10. In 1997, Eggink et al. first reported a keratitis case caused by N. farcinica in a patient using improperly cleaned contact lenses5. A study conducted on 138 patients with eye infections caused by Nocardia from 1999 to 2010 by DeCroos et al. (2011) also showed that the majority of eye infections caused by Nocardia were keratitis (111/138 patients); the remainder were conjunctivitis and endophthalmitis. This was also the largest report of ocular Nocardia infection but only 6/111 patients had N. farcinica isolates, and most cases of keratitis were caused by N. asteroides (51/111 cases)3.
The most common risk of Nocardia keratitis is traumatic corneal damage; other recognized risks include surgery (LASIK, PHACO, etc.), prolonged use of topical corticosteroids, and wearing contact lenses11, and can occur in patients with normal immune systems. DeCroos et al. (2011) also showed that all patients with Nocardia keratitis had no previous history of disease that may cause immune system deficiency3. The majority of patients with Nocardia keratitis have a history of ocular exposure to soil, plants, or agriculture-related occupations3. Approximately half of patients are considered to have Nocardia keratitis upon examination if there are characteristic corneal symptoms such as patchy anterior stromal infiltrates with yellow-white pin-head-sized raised calcareous lesions arranged in a wreath pattern7. Infiltration is often located in the mid-periphery of the cornea near the site of damage or abrasion11. Clinically, Nocardia keratitis can be confused with fungi or atypical mycobacteria. In this patient, eye symptoms appeared around one week after lens replacement surgery. Immediately after surgery, the patient returned to farming work and these symptoms may be similar to the irritation after lens replacement, so the patient was treated with corticosteroid eyedrops for two months. There is a risk that prolonged Nocardia keratitis may lead to corneal abscesses or not be recorded in patients with previous immunodeficiency diseases.
Based on phenotypic characteristics such as bacterial morphology, a positive Gram stain can indicate Nocardia or some aerobic actinomycetes with similar morphology. DeCroos et al.(2011) showed that Gram staining can detect about 63% of cases of Nocardia keratitis early3. In this patient, the presence of bacteria was not recorded in the Gram stain smear-directed sample, which may be due to the patient having an onset three months before hospitalization and using antibiotics, anti-inflammatories, and corticosteroid eyedrops. However, Nocardia species have different epidemiological characteristics, toxins, and antibiotic sensitivities, so accurate species identification is important in choosing the appropriate treatment. To accurately identify Nocardia species, it is necessary to culture specimens and use appropriate identification methods. Currently, most clinical microbiology laboratories use biochemical tests to identify microorganisms, but Nocardia grows slowly and identification often takes a long time and can be inaccurate, because there are many newly isolated Nocardia species, and the biochemical characteristics of the species in the reports are not consistent10. The identification by protein mass spectrometry technology (MALDI-TOF MS) can give quick and accurate results for many Nocardia species that often cause disease10; however, not many microbiology laboratories in Viet Nam use this system. In our study, we used the VITEK-MS system of Biomerieux (Marcy-l'Étoile, France) to identify the isolated agent as N.farcinica. In addition, molecular biology methods or gene sequencing can be used to identify cases that cannot be identified by the MALDI-TOF method, but the technique is complex and expensive, so it is difficult to apply in clinical microbiology laboratories. Regarding antibiogram testing, due to the slow growth of bacteria, the microdilution method in liquid medium is the gold standard for determining the antibiotic sensitivity level of Nocardia. However, this technique is complex and rarely used in clinical laboratories, so most clinical microbiology laboratories only report identification results, and clinicians can choose antibiotics according to the normal susceptibility spectrum of bacteria and according to treatment guidelines. According to the standards of the Clinical and Laboratory Standards Institute (CLSI), N. farcinica is often sensitive to amikacin, amoxicillin-clavulanic acid, ciprofloxacin, linezolid, and sulfonamides and resistant to ceftriaxone, clarithromycin, and tobramycin. Reports of keratitis indicate that Nocardia usually responds well to aminoglycosides and sulfonamides7, of which ophthalmic amikacin is considered the first choice of treatment, followed by tobramycin and gentamicin12. Sensitivity rates to amikacin, gentamicin, and gatifloxacin of Nocardia in 111 cases of keratitis were also relatively high (97%, 85%, and 75% respectively)3.
Conclusion
We report the first case of keratitis after PHACO surgery due to N. farcinica. Because the frequency of the disease is rare and symptoms that occur immediately after surgery can overlap with postoperative irritation, clinicians need to pay attention to the patient's risk factors, such as contact with soil or dust immediately after surgery, characteristic clinical signs, and the response to common treatment methods to guide diagnosis, and patient samples should be tested to find the pathogen. However, because Nocardia exists commonly in nature, there needs to be a discussion between the laboratory and the clinician to determine the meaning of Nocardia isolated in samples.
Abbreviations
AFB: Acid Fast Bacilli, HIV: Human Immunodeficiency Virus
Acknowledgments
The authors would like to thank the patient for his support in this case report.
Author’s contributions
Conceptualization and Investigation: MLP, TVNA; Writing-Original Draft: MLP, VDTT, PTT; Writing-Review & Editing: all authors. All authors read and approved the final manuscript.
Funding
None.
Availability of data and materials
Data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
References
-
Zhang
Z.,
Cao
K.,
Liu
J.,
Wei
Z.,
Xu
X.,
Liang
Q.,
Pathogens and antibiotic susceptibilities of global bacterial keratitis: a meta-analysis. Antibiotics.
2022;
11
(2)
:
238
.
View Article Google Scholar -
Soleimani
M.,
Masoumi
A.,
Khodavaisy
S.,
Heidari
M.,
Haydar
A.A.,
Izadi
A.,
Current diagnostic tools and management modalities of Nocardia keratitis. Journal of Ophthalmic Inflammation and Infection.
2020;
10
(1)
:
36
.
View Article PubMed Google Scholar -
DeCroos
F.C.,
Garg
P.,
Reddy
A.K.,
Sharma
A.,
Krishnaiah
S.,
Mungale
M.,
Hyderabad Endophthalmitis Research Group
Optimizing diagnosis and management of nocardia keratitis, scleritis, and endophthalmitis: 11-year microbial and clinical overview. Ophthalmology.
2011;
118
(6)
:
1193-200
.
View Article PubMed Google Scholar -
Nocard
E.,
Note sur la maladie des boeufs de Guadeloupe connue sous le nom de farcin. Ann Inst Pasteur.
1888;
2
:
293-302
.
-
Eggink
C.A.,
Wesseling
P.,
Boiron
P.,
Meis
J.F.,
Severe keratitis due to Nocardia farcinica. Journal of Clinical Microbiology.
1997;
35
(4)
:
999-1001
.
View Article PubMed Google Scholar -
Conville
P.S.,
Witebsky
F.G.,
Nocardia, Rodococcus, Gordonia, Actinomadura, Streptomyces, and other aerobic actinomycetes. 2015;
:
505-35
.
View Article Google Scholar -
Garg
P.,
Fungal, Mycobacterial, and Nocardia infections and the eye: an update. Eye (London, England).
2012;
26
(2)
:
245-51
.
View Article PubMed Google Scholar -
Wang
H.,
Zhu
Y.,
Cui
Q.,
Wu
W.,
Li
G.,
Chen
D.,
Epidemiology and Antimicrobial Resistance Profiles of the Nocardia Species in China, 2009 to 2021. Microbiology Spectrum.
2022;
10
(2)
.
View Article PubMed Google Scholar -
Cordioli
G.,
Di Pietra
G.,
Asa'ad
S.,
Meneghello
S.,
Del Vecchio
C.,
De Canale
E.,
Nocardia infections in Italy: from a local to a national view. The New Microbiologica.
2023;
46
(1)
:
68-74
.
PubMed Google Scholar -
Conville
P.S.,
Brown-Elliott
B.A.,
Smith
T.,
Zelazny
A.M.,
The Complexities of Nocardia Taxonomy and Identification. Journal of Clinical Microbiology.
2017;
56
(1)
.
View Article PubMed Google Scholar -
Sridhar
M.S.,
Sharma
S.,
Reddy
M.K.,
Mruthyunjay
P.,
Rao
G.N.,
Clinicomicrobiological review of Nocardia keratitis. Cornea.
1998;
17
(1)
:
17-22
.
View Article PubMed Google Scholar -
Lalitha
P.,
Nocardia keratitis. Current Opinion in Ophthalmology.
2009;
20
(4)
:
318-23
.
View Article PubMed Google Scholar
Comments
Article Details
Volume & Issue : Vol 11 No 2 (2024)
Page No.: 6198-6202
Published on: 2024-02-29
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 3248 times
- PDF downloaded - 1128 times
- XML downloaded - 85 times
