

Exploring Variations in Platelet-Rich Plasma Content among Different Preparation Kits
- University of Santo Tomas, España, Manila, Philippines
Abstract
Introduction: The clinical potential of platelet-rich plasma (PRP) has prompted extensive research into its composition and mechanisms of action in regenerative medicine. This study aimed to evaluate and compare the cellular profiles and growth factor concentrations of PRP prepared using three commercially available kits (designated A, B, and C).
Methods: PRP was isolated from fifteen healthy volunteers. The Wilcoxon signed-rank test was used to assess differences between baseline hematological parameters and post-processing values. Subsequently, the cellular and growth factor content of the respective preparations were compared using the Kruskal-Wallis test.
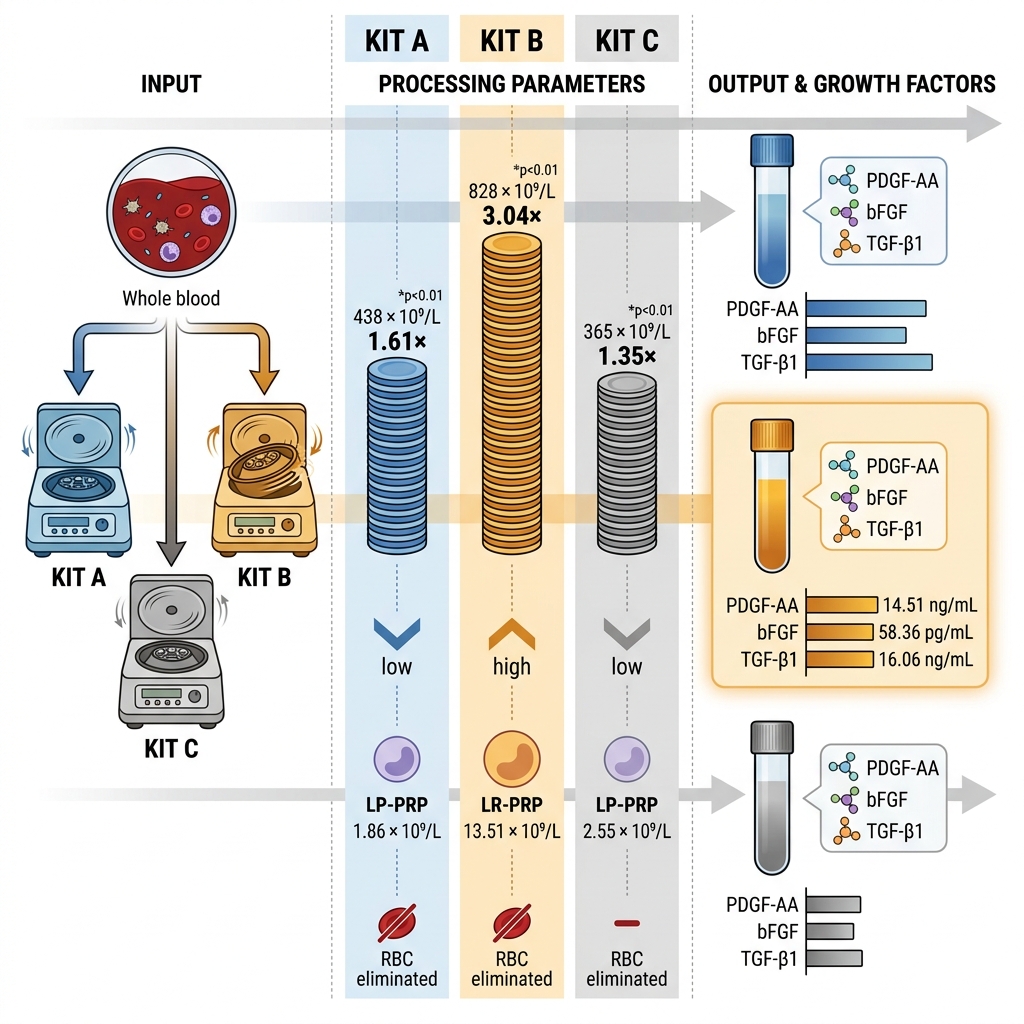
Results: Our findings indicate significant heterogeneity in the cellular and growth factor profiles of PRP isolated using the three kits. Specifically, the white blood cell (WBC) concentration in PRP isolated using Kit B was significantly higher than that observed in preparations from Kits A and C. Although all three kits demonstrated a significant increase in platelet concentrations relative to baseline, the fold-increases varied: 1.61-fold (Kit A), 3.04-fold (Kit B), and 1.35-fold (Kit C). Regarding growth factor concentrations, significantly elevated levels of PDGF-AA, bFGF, and TGF-β1 were observed in PRP isolated using Kit B compared to Kits A or C; conversely, PDGF-BB and IGF-1 values were comparable across all groups.
Conclusion: These variations demonstrate that disparities in PRP preparation protocols directly influence the cellular and molecular composition of the final product. While each kit successfully concentrated platelets, characterizing these differences in cellular and growth factor content is essential for optimizing treatment efficacy. Tailoring PRP preparation protocols to achieve specific cellular and growth factor profiles may be necessary to optimize outcomes for distinct clinical applications. Further investigation into the standardization of PRP preparation for specific therapeutic indications is warranted.
Introduction
Platelet-rich plasma (PRP) is increasingly utilized as an alternative therapeutic modality for various health conditions 1,2. Platelets, the primary bioactive component of PRP, secrete growth factors necessary for wound healing and tissue repair 1,2. The majority of the hemostatic capacity of platelets is associated with their alpha (α)-granules, one of three types of secretory granules found in the platelet cytoplasm 3. Contained within these α-granules are several growth factors, such as platelet-derived growth factor (PDGF), insulin-like growth factor 1 (IGF-1), basic fibroblast growth factor (bFGF), and transforming growth factor-beta (TGF-β) 3. These growth factors promote mitogenesis, angiogenesis, and extracellular matrix (ECM) remodeling of connective tissues 3.
While platelets play vital roles in hemostasis and wound healing, the growth factors stored within platelet α-granules also exert therapeutic effects on diverse tissue types 3. PDGFs promote fibroblast proliferation, thereby improving ECM formation and increasing collagen synthesis 4,5. IGF-1, a potent mitogenic growth factor, stimulates cell growth by modulating nutrient uptake and regulating cell proliferation 6,7. bFGF promotes stem cell proliferation and renewal via the ERK pathway 8. TGF-β1, the most abundant isoform of TGF-β, exerts pleiotropic effects on connective tissue, specifically facilitating growth and differentiation via fibroblast proliferation 9,10,11.
It is important to note that while PRP is employed for various musculoskeletal disorders, differences in leukocyte profiles may influence tissue-specific healing responses 12. Several PRP preparations allow for the retention of leukocytes, as several cytokines released by these cells are regenerative and anti-inflammatory 12. During tissue injury, neutrophils are recruited to the site of injury, promoting local inflammation and apoptosis through the release of cytokines such as IL-1, TNF-α, proteases, and reactive oxygen species (ROS) 13. These primarily serve to clear the area of damaged tissue and infected cells, but may induce collateral damage to healthy tissue when present in excess 13. In addition, the production and release of ROS further promote tissue injury and perpetuate local inflammatory response 14. Monocytes and macrophages primarily remove cellular debris and pathogenic substances through phagocytosis, but these also release cytokines like IL-1 and TNF-α 15,16. Excessive inflammation may lead to fibrosis or scar tissue formation, which fails to provide the structural integrity, elasticity, and overall homeostasis characteristic of healthy tissue 17,18. Leukocyte-rich PRP (LR-PRP) may be beneficial for the rehabilitation of tissue types with inherently poor vascularization, such as tendons 19 and cartilage 20. Conversely, degenerative pathologies, such as those involving chronic inflammation, may react more favorably to a PRP product that does not promote further inflammation, such as leukocyte-poor PRP (LP-PRP) 21. Several systematic reviews and clinical trials recommend LP-PRP for degenerative disorders like osteoarthritis 21, while LR-PRP is recommended for conditions involving tendon pathologies and tears 22,23.
The regenerative effects of platelet-derived growth factors make PRP an attractive therapeutic for treating many health conditions 24. Although PRP is being adopted for use in healthcare systems, commercially available PRP kits differ in their preparation procedures. However, differences in these preparation procedures result in variations in cellular components, which may lead to differences in utility and efficacy. Thus, this study aims to compare three commercially available PRP kits based on the blood cell content and growth factor concentrations present in the PRP isolated using the three kits.
Methodology
Participant Recruitment
To minimize biological variability that could affect the composition of the PRP product, only male participants aged 18–45 years were recruited as potential donors. Written informed consent was obtained from all participants prior to enrollment in accordance with the protocol approved by the Institutional Ethics Committee (FOPREC-2122-119). All procedures were performed in compliance with the ethical standards of the Declaration of Helsinki. Prospective participants completed a health assessment questionnaire to determine eligibility. Vital signs were recorded for all participants; individuals presenting with abnormalities were excluded and referred to a physician for further evaluation and management. Anthropometric measurements (height and weight) were obtained, and body mass index (BMI) was calculated. Only individuals with a normal BMI (defined by the World Health Organization classification as 18.5–24.9) were eligible for inclusion in the study.
Specific exclusion criteria were established to mitigate potential bias and variability. Candidates were excluded if they met any of the following criteria: a history of blood transfusion, organ transplant, or previous PRP, stem cell, and/or growth factor therapy; pre-existing metabolic disorders, malignancies, or transfusion-transmissible infections; or a history of heavy smoking, alcohol misuse, substance abuse, and/or the use of performance-enhancing drugs.
Additionally, complete blood count (CBC) was determined and assessed before inclusion in the study as part of the screening procedures. Briefly, three (3) mL of blood were collected and placed in a vacuum tube containing ethylene diamine tetraacetic acid (EDTA). CBC values were measured using an automated hematology analyzer (Pentra ES60, Horiba, Japan). CBC values required for participation are the following: red blood cell concentration between 4.5-6.0 x 10/L; blood hemoglobin of at least 14.0 g/dL; white blood cell concentration between 4.5-11.0 x 10/L; and platelet concentration between 200-400 x 10/L. Participants with CBC results that did not meet the required values were not included in the study. A total of 15 participants were included in the study (computed using G*Power 3.1.9.7, using an effect size of 0.5, a 0.05, and power of 0.80).
PRP Preparation
Whole blood was collected via venipuncture of the median cubital vein using a butterfly needle. PRP products were prepared strictly according to the manufacturer’s instructions. In addition, whole blood collected in an EDTA tube was utilized to establish baseline CBC values.
The preparation protocols for the three kits are described as follows:
-
PRP Kit A employs a double-syringe system, in which the outer syringe serves as both the blood collection and separation device. After centrifugation, the inner syringe plunger is retracted to collect the supernatant PRP.
-
PRP Kit B utilizes a "push-system" separation device. Following blood collection in a 15-mL syringe, the sample is transferred into the separation device for centrifugation. Post-centrifugation, a screw mechanism is employed to push the contents upward, facilitating the collection of the topmost platelet-poor plasma (PPP) and the buffy coat layer containing the PRP.
-
PRP Kit C utilizes a blood collection tube incorporating a separator gel. Nine milliliters (9 mL) of blood is collected and transferred directly to the tube for centrifugation. During this process, the separator gel migrates to create a physical barrier between the heavier erythrocytes and leukocytes and the lighter platelets and plasma. The resulting PRP is then collected using a syringe.
The procedural differences among the three kits are summarized in Table 1. To maintain analytical blinding, all prepared PRP samples were anonymized and randomized prior to analysis, ensuring that personnel performing the CBC and ELISA measurements were masked to the kit of origin.
Methods of PRP Preparation using Three Commercially Available PRP Kits
| Parameters | PRP Preparation Kit | ||
|---|---|---|---|
| PRP Kit A | PRP Kit B | PRP Kit C | |
| Separation System Used | Double syringe | Push system | Gel-based system |
| Anticoagulant | ACD-A | Sodium citrate | Sodium citrate |
| Volume of anticoagulant | 1.5 mL | 1.5 mL | 1 mL |
| Volume of whole blood collected (mL) | 13.5 mL | 13.5 mL | 9 mL |
| Number of centrifugation steps | 1 | 1 | 1 |
| Centrifugation speed | 300 x | 1,700 x | 1,500 x |
| Centrifugation time | 10 minutes | 5 minutes | 10 minutes |
| Removal of platelet-poor plasma (PPP) | No | Yes | No |
| Volume of PRP | 8 mL | 1 mL | 5 mL |
Hematological Analysis
The CBC parameters of baseline whole blood and PRP isolated using Kit A, Kit B, and Kit C were measured using an automated hematology analyzer machine (Pentra ES 60, Horiba, Japan). This machine used impedance technology to measure concentrations and create histograms of the RBCs, WBCs, and platelets present in the sample, based on cell size. Hemoglobin was measured using a modified cyanmethemoglobin method. RBC indices were computed by the automated hematology analyzer based on the measured CBC and hemoglobin values. To assess the degree of change in RBC, WBC, and platelet counts in PRP compared with baseline values, the following formulas were used:
Growth Factor Measurements
After preparation, the homogenous PRP prepared using the three commercially available PRP kits were collected and used to measure growth factors via sandwich ELISA. The following ELISA test kits were used: FineTest Human PDGF-AA ELISA Kit (EH3532, Wuhan Fine Biotech, China), FineTest Human PDGF-BB ELISA Kit (EH0254, Wuhan Fine Biotech, China), FineTest Human IGF-1 ELISA Kit (EH0165, Wuhan Fine Biotech, China), FineTest Human FGF2 ELISA Kit (EH0541, Wuhan Fine Biotech, China), and FineTest Human TGF-β1 ELISA Kit (EH0287, Wuhan Fine Biotech, China). Measurement of OD 450 was performed using the FluoStar Omega spectrophotometer (BMG Labtech, Germany).
Statistical Analysis
A combination of Microsoft Excel and GraphPad Prism version 10.2.0 was used in the study. Descriptive statistics were used to demonstrate the CBC and growth factor levels measured during the in vitro analysis. The Wilcoxon signed-rank test was used to compare CBC parameters of PRP isolated using each kit with baseline whole blood CBC values. The Kruskal-Wallis test assessed the difference in the CBC and growth factor levels obtained using the three commercially available PRP Kits. Pairwise comparisons using corrected Dunn’s test were performed to determine the difference in the CBC and growth factor levels among each PRP preparation. Finally, Spearman r correlation was performed to describe the relationship between growth factor measurements with WBC and PRP concentrations. All p-values less than or equal to 0.05 are considered statistically significant.
Results
The demographic data of the fifteen patients are shown in Table 2. All prospective participants interviewed (n = 15) registered normal vital signs. Screening CBC values were also within normal limits (data not shown).
Patient Demographic Characteristics
| Demographic Profile | Participants mean ± SD (95% CI) |
|---|---|
| Age (years) | 28.1 ± 7.2 (21.2 – 34.9) |
| Weight (kg) | 63.2 ± 9.9 (50.2 – 76.2) |
| Height (m) | 1.7 ± 0.1 (1.6 – 1.8) |
| BMI | 22.6 ± 2.0 (22.0 – 23.1) |
| BMI category | Normal |
| Systolic Blood Pressure (mmHg) | 113.3 ± 8.7 (103.5 – 123.2) |
| Diastolic Blood Pressure (mmHg) | 84.3 ± 9.0 (73.6 – 94.9) |
Table 3 shows the mean CBC values of the three different PRP preparations, the Wilcoxon signed-rank test results of mean whole blood CBC values versus each of the three PRP kits, and the Kruskal-Wallis test results comparing each of the three PRP kits. All three PRP kits had significantly lower RBC concentrations compared to whole blood. When compared with baseline RBC values, on average, PRP produced by PRP Kit A has 0.01 times less RBCs, PRP Kit B produced PRP with 0.04 times less RBCs, and PRP from PRP Kit C reported the greatest reduction in RBCs, with 0.003 times less RBCs with baseline. These findings suggest effective separation of RBCs from the PRP product by the PRP kits (p values <0.01) .
When comparing WBC measurements of the prepared PRP samples with baseline whole blood values, significantly lower mean ± SD WBC concentrations were observed in PRP isolated using Kit A (Baseline 7.61 x 10/L ± 1.68 vs Kit A 1.86 x 10/L ± 0.85; p <0.01) and using Kit C (Baseline 7.61 x 10/L ± 1.68 vs Kit C 2.55 x 10/L ± 1.28; p <0.01), while PRP isolated using Kit B resulted in higher overall WBC concentration (Baseline 7.61 x 10/L ± 1.68 vs Kit B 12.86 x 10/L ± 12.52; p 0.41). Based on the classification of Kon et al. 25, PRP with WBC concentrations less than baseline whole blood values are considered LP-PRP, while PRP with WBC concentrations greater than baseline values are considered LR-PRP. Considering this, Kits A and C produced PRP, as they were able to decrease WBC concentrations by 0.25 times and 0.34 times compared with baseline, respectively (p values <0.01). Meanwhile, PRP Kit B produced LR-PRP with 1.90 times more WBCs compared with baseline (p 0.41) .
Table 3 also shows that varying WBC differential profiles were observed from the PRP isolated using the three kits. Compared with baseline whole blood values, the three kits reported significantly lower relative neutrophil values (Whole Blood 56.41 % ± 9.59; PRP Kit A 31.24 % ± 12.05; PRP Kit B 44.51 % ± 13.77; PRP Kit C 8.76 % ± 1.85). Inversely, relative lymphocyte concentrations were also significantly increased in PRP prepared using the three kits compared with baseline whole blood measurements (Whole Blood 35.25 % ± 8.65; PRP Kit A 62.88 % ± 13.15; PRP Kit B 48.93 % ± 13.96; PRP Kit C 85.35 % ± 3.17). All PRP preparations also resulted in significant decreases in relative concentrations of monocytes, eosinophils, and basophils compared to whole blood values. Regardless of the relative WBC differential concentrations for each PRP, the use of PRP Kit B resulted in significantly higher absolute WBC differential concentrations than using PRP Kit A and C (data not shown), due to PRP Kit B producing a PRP rich in leukocytes.
Finally, PRP isolated using the three PRP kits showed significant increases in their platelet concentrations. PRP isolated using PRP Kit A resulted in a 1.61-fold increase in platelet concentration (Baseline 273 x 10/L ± 43 vs Kit A 438 x 10/L ± 75; p <0.01*). Meanwhile, PRP isolated using PRP Kit B resulted in a 3.04-fold increase in platelet concentration (Baseline 273 x 10/L ± 43 vs Kit B 828 x 10/L ± 424; p < 0.01*). Finally, PRP isolated using PRP Kit C resulted in a 1.35-fold increase in platelet concentration (Baseline 273 x 10/L ± 43 vs Kit C 365 x 10/L ± 46; p <0.01*).
Comparison of measured CBC values in Whole Blood vs PRP isolated using PRP kits A, B, and C
| CBC Parameters |
Baseline Whole Blood Mean ± SD (95% CI) | Baseline Whole Blood vs PRP isolated using Kit A | Baseline Whole Blood vs PRP isolated using Kit B | Baseline Whole Blood vs PRP isolated using Kit C |
Kruskal-Wallis Test (PRP isolated using Kits A, B, & C) | ||||
|---|---|---|---|---|---|---|---|---|---|
|
PRP isolated using Kit A Mean ± SD (95% CI) |
PRP isolated using Kit B Mean ± SD (95% CI) |
PRP isolated using Kit C Mean ± SD (95% CI) | |||||||
| RBC (x1012/L) |
4.53 ± 1.29 (3.82 – 5.25) |
0.06 ± 0.09 (0.01 – 0.12) | <0.01* |
0.18 ± 0.32 (0.01 – 0.36) | <0.01* |
0.02 ± 0.01 (0.01 – 0.02) | <0.01* | 16.13 | <0.01* |
| RBC Increase Factor | 1.00 ± 0.00 |
0.01 ± 0.01 (0.00 – 0.02) | <0.01* |
0.04 ± 0.07 (0.002 – 0.08) | <0.01* |
0.003 ± 0.002 (0.002 – 0.004) | <0.01* | 41.19 | <0.01* |
| WBC (x 109/L) |
7.61 ± 1.68 (6.68 – 8.54) |
1.86 ± 0.85 (1.39 – 2.33) | <0.01* |
13.51 ± 12.52 (6.57 – 20.44) | 0.41 |
2.55 ± 1.28 (1.84 – 3.26) | <0.01* | 15.88 | <0.01* |
| WBC Increase Factor | 1.00 ± 0.00 |
0.25 ± 0.13 (0.18 – 0.32) | <0.01* |
0.90, 2.97 (0.45, 3.42)^ | 0.82 |
0.34 ± 0.17 (0.25 – 0.44) | <0.01* | 34.41 | <0.01* |
| Neutrophil (%) |
56.40 ± 9.59 (51.08 – 61.72) |
31.24 ± 12.05 (24.57 – 7.91) | <0.01* |
44.51 ± 13.77 (36.88 – 2.13) | <0.01* |
8.76 ± 1.85 (7.74 – 9.79) | <0.01* | 30.07 | <0.01* |
| Lymphocyte (%) |
35.25 ± 8.65 (30.46 – 40.04) |
62.88 ± 13.15 (55.60 – 0.17) | <0.01* |
48.93 ± 13.96 (41.20 – 6.67) | <0.01* |
85.35 ± 3.17 (83.60 – 7.11) | <0.01* | 28.07 | <0.01* |
| Monocyte (%) |
6.60 ± 1.59 (5.71 – 7.49) |
3.94 ± 1.33 (3.20 – 4.67) | <0.01* |
4.59 ± 1.4 (3.79 – 5.39) | 0.01* |
4.74 ± 2.02 (3.62 – 5.86) | 0.02* | 4.02 | 0.13 |
| Eosinophil (%) |
2.90 ± 2.22 (1.67 – 4.13) |
1.62 ± 1.01 (1.06 – 2.18) | 0.02* |
1.41 ± 0.81 (0.83 – 1.99) | <0.01* |
0.22 ± 0.13 (0.15 – 0.29) | <0.01* | 21.08 | <0.01* |
| Basophil (%) |
1.08 ± 0.37 (0.87 – 1.29) |
0.32 ± 0.18 (0.22 – 0.42) | <0.01* |
0.56 ± 0.39 (0.34 – 0.78) | 0.01* |
0.49 ± 0.16 (0.39 – 0.58) | <0.01* | 8.12 | 0.02* |
| Platelet (x 109/L) |
273 ± 43 (250 – 298) |
438 ± 75 (396 – 480) | <0.01* |
828 ± 424 (593 – 1064) | <0.01* |
365 ± 46 (339– 390) | <0.01* | 13.94 | 0.01* |
| Platelet Increase Factor | 1.00 ± 0.00 |
1.61 ± 0.27 (1.47 – 1.76) | <0.01* |
3.04 ± 1.60 (2.16 – 3.93) | <0.01* |
1.35 ± 0.21 (1.24 – 1.47) | <0.01* | 13.68 | <0.01* |
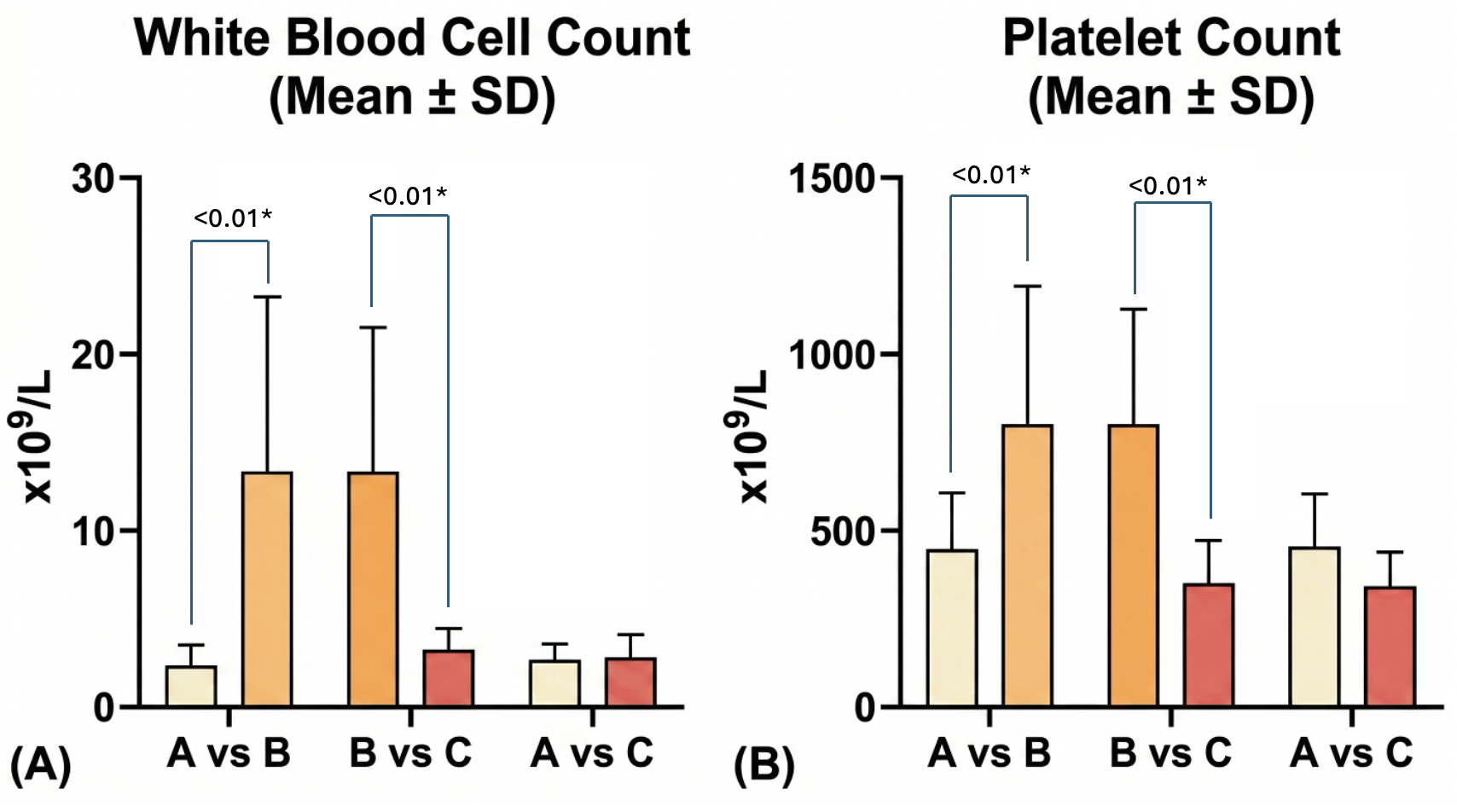
Pairwise comparisons of white blood cell concentration and platelet concentration of PRP isolated using Kits A, B, and C. Abbreviations: A – PRP Kit A, B – PRP Kit B, C – PRP Kit C, SEM – standard error of the mean; Error bars indicate standard error of the mean (SEM)
Pairwise comparisons (results shown in Figure 1) performed post-hoc the Kruskal-Wallis test shows that PRP isolated using Kit B produced higher WBC concentrations than Kits A and C (seen in Figure 1a), as well as significantly higher platelet concentrations (seen in Figure 1b). Amongst all PRP preparations, PRP isolated using Kit B performed best at concentrating WBCs and platelets in PRP.
Table 4 shows the comparison of mean growth factor measurements of the three PRP preparations. Among all PRP preparations, significant variations in the concentrations of PDGF-AA (p <0.01) was observed, while variations in concentrations of PDGF-BB, IGF-1, and TGF-β values were nonsignificant.
Comparison of growth factor concentrations present in PRP isolated using PRP kits A, B, and C
| Growth Factor Parameters | Mean ± SD (95% CI) | Kruskal-Wallis Test | |||
|---|---|---|---|---|---|
| PRP isolated using Kit A | PRP isolated using Kit B | PRP isolated using Kit C | |||
| PDGF-AA (ng/mL) |
11.66 ± 2.69 (10.17 – 13.15) |
14.51 ± 2.00 (13.30 – 15.72) |
12.90 ± 1.43 (12.04 – 13.76) | 17.28 | |
| PDGF-BB (ng/mL) |
24.17 ± 8.17 (19.65 – 28.70) |
26.65 ± 11.68 (20.18 – 33.11) |
25.61 ± 9.42 (20.39 – 30.83) | 3.70 | 0.29 |
| IGF-1 (ng/mL) |
71.83 ± 17.68 (61.15 – 82.52) |
83.09 ± 22.44 (70.13 – 96.04) |
85.22 ± 35.14 (63.99 – 106.50) | 2.45 | 0.48 |
| bFGF (pg/mL) |
41.24 ± 12.12 (34.53 – 47.96) |
58.36 ± 29.51 (39.61 – 77.11) |
37.81 ± 7.65 (33.39 – 42.22) | 6.11 | 0.05* |
| TGF- β1 (ng/mL) |
8.81 ± 3.24 (6.94 – 10.68) |
16.06 ± 14.23 (7.02 – 25.10) |
7.27 ± 2.25 (6.02 – 8.51) | 5.23 | 0.07 |
Growth factor content was measured in PRP isolated using each of the three kits. As seen in Figure 2a, PRP isolated using Kit B had significantly higher PDGF-AA values than PRP isolated using Kit A (p <0.01) and PRP isolated using Kit C (p 0.03). Figure 2d shows PRP isolated using Kit B also produced significantly higher bFGF values than PRP isolated using Kit A (p 0.05) and PRP isolated using Kit C (p 0.05). Figure 2e shows that PRP prepared using PRP Kit B had significantly higher TGF- β1 values than PRP isolated using Kit C (p 0.03*). PDGF-BB (Figure 2b) and IGF-1 (Figure 2c) values were comparable amongst all preparations.
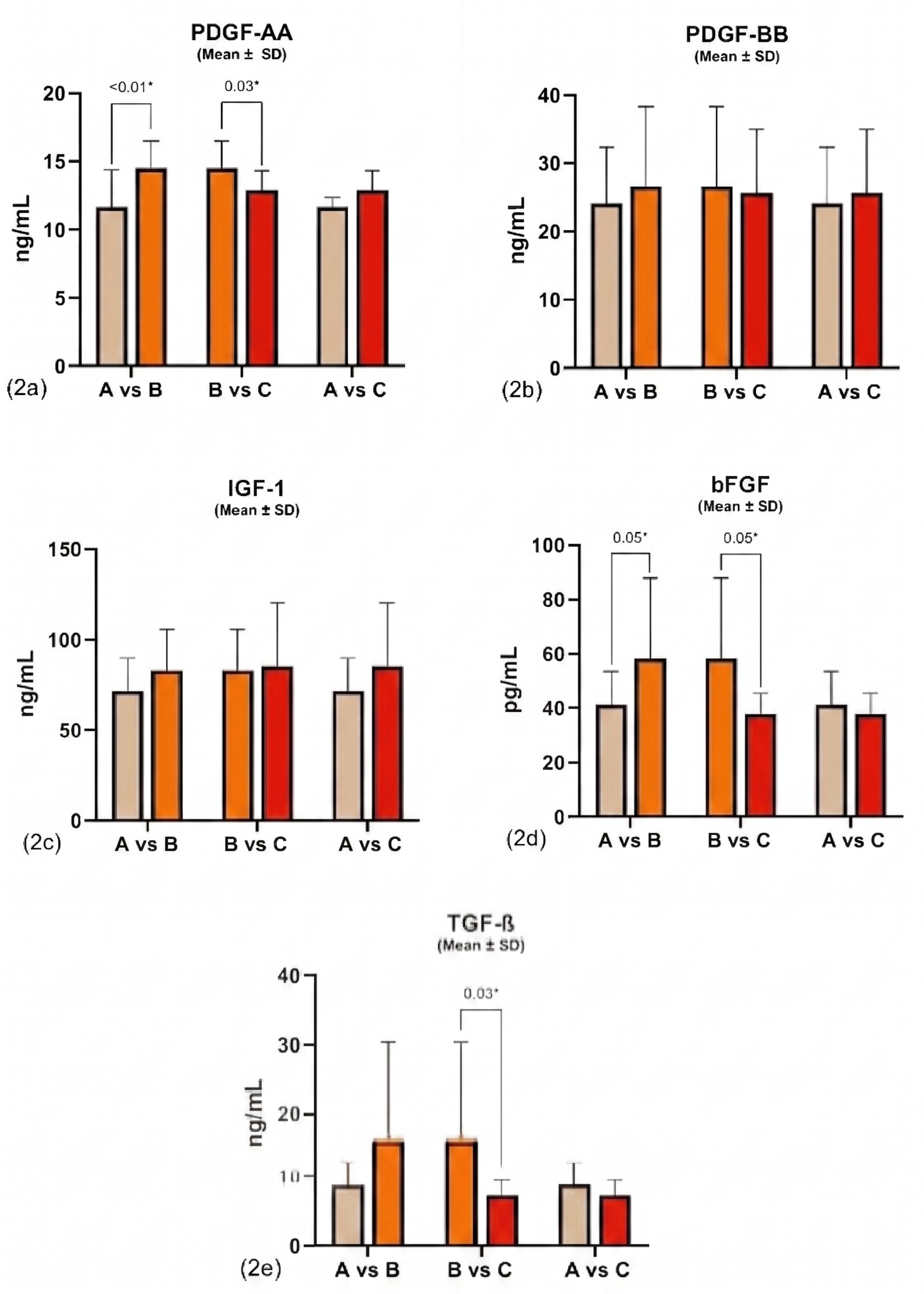
Pairwise comparisons of growth factor concentrations in PRP isolated using Kits A, B, and C
Spearman r correlation was performed to assess the relationship of measured growth factors with WBC concentration (shown in Table 5) and with platelet concentration (shown in Table 6). PDGF-AA, PDGF-BB, and TGF- β1 values exhibited significant positive correlations with both WBC and platelet concentrations. Correlations between the three growth factors and platelet concentration were higher than with WBC concentration, suggesting that the number of platelets in PRP may have a greater impact in the levels of PDGF-AA, PDGF-BB, and TGF- β1 than the number of WBCs. Meanwhile, the relationship of bFGF was only significant with WBC concentration, suggesting that PRP with higher WBC concentrations may result in a PRP product with greater bFGF concentrations. Finally, there were no significant relationships observed between IGF-1 and either WBC or platelet concentrations.
Relationship between WBC concentration and growth factor measurement
| Spearman r | Correlation with WBC concentration | Correlation with Platelet concentration | ||
|---|---|---|---|---|
| Spearman r (95% CI) | Spearman r (95% CI) | |||
| PDGF-AA |
0.53 (0.25 to 0.72) | <0.01* |
0.57 (0.30 to 0.75) | <0.01* |
| PDGF-BB |
0.52 (0.09 to 0.60) | <0.01* |
0.45 (0.17 to 0.66) | <0.01* |
| IGF-1 |
0.24 (-0.08 to 0.51) | 0.15 |
0.23 (-0.09 to 0.51) | 0.15 |
| bFGF |
0.32 (0.02 to 0.57) | 0.04* |
0.16 (-0.17 to 0.45) | 0.32 |
| TGF- β1 |
0.34 (0.02 to 0.58) | 0.03* |
0.58 (0.34 to 0.76) | <0.01* |
Discussion
This study shows that all PRP preparation kits tested produced a final product with significantly increased platelet concentration, with PRP isolated using Kit B yielding the highest platelet concentration per preparation. RBC concentrations were also significantly lower than baseline across all PRP preparations, resulting in markedly decreased hemoglobin and hematocrit values (not shown), suggesting efficient separation. However, WBC concentrations differ among all preparations. PRP isolated using Kits A and C reported WBC concentrations lower than baseline, while PRP isolated using Kit B resulted in higher WBC concentrations.
Differences in the blood cell concentrations and profiles of PRP products can be attributed to the different preparation parameters amongst published PRP protocols, which lead to heterogeneity in observed measurements 26. First, both the total amount of blood collected and the final amount of PRP differ among each PRP preparation kit. Both Kit A and Kit B require 13.5 mL of blood to prepare PRP, and Kit C requires only 9 mL of blood. Unsurprisingly, Kit C produced the lowest platelet concentration in the final PRP product. The volume of PRP obtained using Kit A is 8 mL; using Kit B, 1 mL of PRP and 7 mL of PPP (platelet-poor plasma) was obtained; and using Kit C, 5 mL of PRP was obtained. Although the volume of PRP is essential, its efficacy depends on the final platelet concentration delivered. Similarly, for large joints, a precise, targeted approach is used to focus on their therapeutic effect rather than filling the entire joint space; this is usually an ultrasound-guided procedure 27,28.
The volume of PRP to be injected depends on how much injectate volume the area of injury can effectively hold. For small joints such as in the wrist, foot, and ankle, around 2 -3 mL of PRP can be injected, while 5 – 6 mL of PRP can be injected in larger joints such as in the shoulders and knees 29. The volume requirement per injury reiterates the need to modify PRP preparation. If not, cases wherein the PRP volume extracted may be excessive for the area of the injection site, thus, wasting unused PRP. Among the three PRP preparation protocols, only PRP Kit B offers an option of reducing the final volume of PRP extracted and at the same time concentrating the platelet content of the product. When needed, PPP may be combined with the concentrated PRP to effectively fill the area in the injury site.
All three PRP preparation kits were able to concentrate platelets, and each final product meets the definition of PRP as “plasma with a concentration of platelets above the baseline” 25. Among the three PRP kits, PRP Kit B performed the best in concentrating platelets (3.04x baseline values), followed by PRP Kit A (1.61x baseline values), and PRP Kit C (1.35x baseline values). However, the difference in platelet concentrations may influence the extent of the regenerative capacity of the PRP product. A 2019 in vitro study by Wang et al reported cell proliferation in cultures of mesenchymal stem cells (MSCs) that were treated with PRP having a platelet concentration ranging from 200 x 10/L to 1,500 10/L 30. The same study suggests that the optimum concentration to promote cell proliferation was 1,500 x 10/L, as no marked increase in proliferative action was observed in platelet concentrations beyond 1,500 x 10/L, suggesting a ceiling effect on the relationship between PRP concentration and cell proliferation 30.
RBC concentrations were also significantly decreased amongst all PRP preparations. The presence of erythrocytes may damage tissues, as erythrocytes can hemolyze, releasing hemoglobin into the product. Extracellular hemoglobin increases oxidative stress on tissues 31. For instance, free iron released by hemoglobin may act as a catalyst in the formation of hydrogen peroxide, leading to chondrocyte damage and reduction of proteoglycan synthesis, resulting in blood-induced cartilage damage 32. Free hemoglobin may also deplete nitric oxide levels, causing vasoconstriction 33, and potentially decreasing blood flow to the site of injury. Reducing RBC concentrations during PRP preparation greatly minimizes the possible adverse effects of extracellular and extravascular hemoglobin on repairing tissue microenvironment. Because the PRP preparation protocols reported significantly near zero hemoglobin and significantly reduced hematocrit values, the negative effects of hemoglobin on tissue repair are less likely to occur.
In this study, measurement of the WBC concentrations categorizes PRP Kit A (WBC 1.86 x 10/L) and PRP Kit C (WBC 2.55 x 10/L) as kits that can isolate LP-PRP, and PRP Kit B (WBC 13.51 x 10/L) as a kit that can isolate LR-PRP. Being able to identify this, this study also investigated the influence of blood cell components, particularly WBC and platelet components, on growth factor levels. Among the growth factors, only PDGF-AA, PDGF-BB, and TGF-ß1 exhibited moderate relationships with WBC and platelet counts. The study demonstrated that PRP with higher WBC and platelet concentrations corresponded with higher PDGF-AA, PDGF-BB, and TGF-ß1 levels; with platelet concentrations demonstrated to have a greater influence on the levels of these growth factors. While PDGF isomers were originally discovered in platelets, numerous other cellular sources of PDGFs have been discovered, such as macrophages, lymphocytes, and endothelial cells 34. On the other hand, while almost all tissue types produce TGF-ß isomers, TGF-ß1 is mainly produced by immune cells and platelets 35, with platelets notably being the most abundant source36. If the target is to obtain high growth factors, PRP Kit B was able to provide the highest growth factor. It is also important to note that PRP Kit B has high leukocyte count, which may induce inflammation, but the presence of macrophages will help in tissue remodeling and immune modulation. Aside from this, indications of LR-PRP and LP-PRP also varies to avoid such complication, that is, LR-PRP is recommended for chronic conditions like tendinopathy and treatment of bone defects with local dysregeneration, while LP-PRP is for promoting healing with minimal inflammation 37,38,39.
As with bFGF levels, high levels of this growth factor were observed in the three kits but when correlated with WBC concentrations, results showed that its levels are positively correlated with WBC concentrations than platelet concentrations. There could be methodological bias when this is interpreted because from among the three kits, only PRP Kit B produced LR-PRP. Although the 2016 study on WBC and growth factor concentrations in PRP found a negative correlation between WBC and FGF values40, this difference may be influenced by the type of PRP produced. bFGF is shown to promote cell proliferation and angiogenesis that may be beneficial in repairing tendon injuries 41,42.
Finally, IGF-1 is known to be produced in all tissue and cell types, including immune cells 43 and platelets 44. However, this study demonstrated that increases of both WBC and platelet concentrations in PRP did not directly influence IGF-1 levels, corroborating the findings of a 2019 clinical trial regarding PRP use for acute Achilles tendon rupture 45 and those of a 2023 in vitro study on PRP cellular bioactivity 46.
The relationship between growth factors and platelet resulted in different growth factor profiles in PRP produced using the three kits. PRP isolated using Kit B had the highest concentration of PDGF-AA, bFGF, and TGF-β1 values, as well as having slightly higher PDGF-BB values and comparable IGF-1 values. Formation of blood vessels, proliferation of stem cells and fibroblasts, and proper differentiation of connective tissue are all essential in tendon repair and healing 47. However, excessive TGF- β1 activation may induce abnormal deposition of collagen in the ECM 48, leading to the formation of scar tissue. Abnormal scar tissue can reduce muscle contractile function, adversely affecting muscular strength and joint movement 49.
The study acknowledges several limitations. The researchers recognize that the blood content of the final PRP depends on the patient’s baseline blood levels as PRP is an autologous product. Therefore, baseline CBC values are affected by factors such as age or sex. Because of this, the study recruited participants who are males aged 18-45 only, to minimize differences in measured baseline CBC values. Factors such as age or sex may influence CBC values. In 2018, a Korean study on CBC reference intervals show that older populations tend to have decreased WBC and platelet counts 50. The same study also reported that male populations aged 18-45 have significantly higher mean RBC and WBC counts than females, while female populations at the same age range have significantly higher mean platelet counts than males.
The different PRP kits required different amounts of blood to be collected, based on manufacturer specifications. This could affect the absolute CBC values of the final PRP product, as more blood collected and processed would correspond to more platelets in PRP. To better understand the ability of each PRP kit to concentrate platelets from whole blood, the study also presented the factor of change in RBC, WBC, and platelet counts in PRP from baseline values. The usefulness and efficacy of PRP vary significantly in terms of blood cell and growth factor content. Similarly, the applications where PRP can be used require different concentrations of blood cell components and growth factors.
However, because PRP is a patient-specific preparation, the absolute blood cell and growth measurements may not be replicable due to high patient variability, such as age, sex, condition, and initial platelet concentration51. The high biological variability of PRP makes standardizing its content difficult. Nevertheless, there have been calls for standardizing PRP preparation and use. Numerous identified PRP preparation parameters that need standardization include centrifugation parameters (duration, speed, number of times), type of anticoagulant used, and platelet 26,52. Centrifugation parameters can prematurely activate platelets 53, which could influence the release of growth factors. Further studies into the effects of centrifugation on platelet activation via platelet function tests are warranted to fully assess ex vivo activation of platelets during PRP preparation.
The highly technical nature of PRP preparation (ie. careful aspiration for Kit A, or careful screw-pushing for Kit B) relies on the mechanical skill of the clinical staff preparing the PRP, and inconsistencies in skill affect the final PRP content. Reducing the effects on variability of PRP preparation should focus on streamlining PRP preparation by decreasing the reliance on the mechanical skill of the clinical staff in the collection of PRP. Lastly, the results of this study are exploratory, and further correlational studies using a larger sample size could better elucidate the relationship between formed elements and growth factors.
Finally, the study compared the in vitro characteristics of PRP produced using different kits. While measurements in cell values and growth factors via ELISA can potentially characterize the effects of PRP, the study did not assess these effects in vivo. Further studies on in vivo models (ie. cell culture lines or animal models) and measuring values assessing tissue repair function (ie. fibroblast or chondrocyte proliferation) could provide more detailed insights into the effects of different PRP preparation in tissue repair and elucidate the relationships with the effects of PRP as intended.
Identifying the blood cell and growth factor content of PRP prepared with each PRP preparation kit may help physicians choose the best kit for their intended application. As mentioned previously, LP-PRP is recommended for cartilage pathologies, such as degenerative joint disease, while LR-PRP is recommended for tendinopathies and tears. However, practitioners and researchers alike recognize the need for further research and clinical trials on the effectiveness of different PRP types for specific musculoskeletal injuries, further hampered by the lack of standardized PRP protocols 54.
Conclusion
The three PRP kits produced PRP with varying platelet and WBC concentrations. By identifying the CBC profile and growth factor levels in PRP prepared using each PRP preparation protocol, physicians are better able to decide which kit to use for a specific musculoskeletal injury, as some PRP preparations are better suited to a particular type of tissue than others. We recommend that PRP preparation protocols be tailored to the intended clinical application, with kit selection guided by the desired leukocyte and platelet profiles. In addition, studying how adjustments in different PRP preparation methods affect content and mechanisms of action will provide valuable insight that could ultimately contribute to creating standardized and unified PRP preparation methods specific to different medical conditions. Moreover, future studies comparing PRP and its types with other autologous treatments, such as platelet-rich fibrin, may be conducted to expand the range of available alternatives.
Abbreviations
ACD-A: anticoagulant citrate dextrose solution A; BMI: body mass index; bFGF: basic fibroblast growth factor; CBC: complete blood count; CI: confidence interval; ECM: extracellular matrix; EDTA: ethylene diamine tetraacetic acid; ELISA: enzyme-linked immunosorbent assay; g/dL: grams per deciliter; IGF-1: insulin-like growth factor 1; IL-1: interleukin-1; kg: kilogram; LP-PRP: leukocyte-poor platelet-rich plasma; LR-PRP: leukocyte-rich platelet-rich plasma; m: meter; mL: milliliter; mmHg: millimeters of mercury; MSC: mesenchymal stem cell; ng/mL: nanograms per milliliter; OD: optical density; PDGF: platelet-derived growth factor; pg/mL: picograms per milliliter; PPP: platelet-poor plasma; PRP: platelet-rich plasma; RBC: red blood cell; RCF: relative centrifugal force; ROS: reactive oxygen species; SD: standard deviation; SEM: standard error of the mean; TGF-β: transforming growth factor beta; TNF-α: tumor necrosis factor-alpha; WBC: white blood cell; x g: relative centrifugal force.
Acknowledgments
None.
Author’s contributions
All authors read and approved the final manuscript.
Funding
This original article is part of a research program titled "Research Center for the Rehabilitation/Sports Medicine (Oplan Atletang Pinoy)", funded by the Department of Science and Technology—Philippine Council for Health Research and Development (Ref. No. 001911).
Availability of data and materials
Data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
This research study has been granted ethics approval by the University of Santo Tomas Faculty of Pharmacy Research Ethics Committee (UST FOP REC), given the study protocol code FOPREC-2122-119.
Consent for publication
Not applicable.
Declaration of generative AI and AI-assisted technologies in the writing process
The authors declare that they have not used generative AI (a type of artificial intelligence technology that can produce various types of content including text, imagery, audio and synthetic data).
Competing interests
The authors declare that they have no competing interests.