

Pain relief after maxillofacial surgery: efficacy in patients undergoing ultrasound-guided trigeminal nerve block – a randomized controlled trial
- Hanoi medical university, Hanoi, Viet Nam
- Thai Nguyen Medical University, Thainguyen, Viet Nam
- Department of Life Sciences, University of Science and Technology of Hanoi, Viet Nam, Academy of Science and Technology, 18-Hoang Quoc Viet, Cau Giay, Hanoi, Viet Nam
Abstract
Background: Pain management is a critical factor for successful surgical outcomes, as it enables patients to recover more quickly. Maxillofacial surgery is typically complex and requires appropriate pain relief methods. In this study, the use of ultrasound to guide the blocking of the trigeminal nerve was investigated.
Methods: The study enrolled 60 patients in a randomized controlled trial. The patients were divided into two groups: group T received a trigeminal (V) nerve block using ropivacaine under ultrasound guidance; and group C, the control group, received paracetamol infusion. During follow up, the following outcomes were assessed: time required for the first dose of pain relief; 24-hour dose of ketorolac in both groups; visual analog scale (VAS) score at rest and when moving; changes in hemodynamics, including pulse, systolic blood pressure, diastolic and blood pressure and changes in respiration including respiratory rate, and SpO2. Systemic complications such as allergies, anaphylaxis, drug overdose, and anesthetic toxicity, as well as local complications such as vascular puncture, nerve damage, hematoma at the injection site, facial paralysis, jaw dropping, and paresthesia/numbness of the lips and tongue were evaluated.
Results & Conclusion: The results showed that blocking branches V2 and V3 of the trigeminal nerve under ultrasound guidance improved pain relief in patients compared to the intravenous paracetamol. The VAS score of the study group was lower than that of the control group in most cases. In addition, the investigated group could tolerate pain longer until the later first dose of analgesic with a lower dose of ketorolac, which suggests the potential of this intervention in managing pain from maxillofacial surgery.
Introduction
Maxillofacial trauma is a common injury that may result from traffic accidents, injury from daily activities, and severe burns from fire. Oral and maxillofacial surgery for cancer, complex facial fractures, and plastic surgery is becoming increasingly advanced with more sophisticated techniques1. Pain is a common symptom after surgery and is associated with hemodynamic disorders such as tachycardia, increased blood pressure, and tachypnea, as well as increased catecholamine levels, hyperglycemia, and mental disorders. A moderate postoperative pain rate is typically 25% to 35%, and severe pain is 35% to 55%2.
Pain relief therapy after maxillofacial surgery may include cool compresses, intravenous infusion of paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), or intermittent doses of morphine. However, these therapies typically provide only mild to moderate pain relief. Moreover, the duration of pain relief is usually short and can include side effects such as nausea and vomiting, urinary retention, and even respiratory failure3. These side effects can worsen the effect of treatment, particularly in patients who had their jaws wired following maxillofacial surgery. Therefore, the development of new strategies is needed to overcome the disadvantages of conventional pain relief options.
Recently, regional anesthesia has been widely used to increase the effectiveness and duration of postoperative analgesia in patients, as well as reduce undesirable side effects on the hemodynamic and respiratory systems4. Regional anesthesia methods based on anatomical landmarks to reduce pain during maxillofacial surgery are often difficult to carry out because of their complexity and high rate of complications. Ultrasound-guided regional anesthesia has demonstrated many advantages in overcoming this difficulty and has resulted in improved recovery of patients5. In practice, maxillofacial surgery may include wiring the jaw, which inhibits patients from opening their mouth. This may present difficulties in patients given strong pain relievers, such as morphine, which can induce vomiting and nausea.
In the present study, we aimed to investigate whether ultrasound-guided trigeminal nerve blocking could enhance the efficacy of pain relief and to compare the incidence of undesirable side effects to that from conventional methods. We targeted nerves V2 and V3 with a minimal amount of local anesthetic as an effective intervention that could be a significant addition to current clinical practice.
Methods
This study was a prospective, randomized controlled clinical intervention in patients who were undergoing maxillofacial surgery. The study was conducted in the Department of Anesthesiology and Resuscitation and Pain Management, Hanoi Medical University Hospital from October 2019 to October 2020. Ethical permission for this study was obtained from the ethics committee of Thai Nguyen Medical University (Number: 239/ĐHYD-HĐĐĐ). Sixty patients indicated for maxillofacial surgery were recruited. Inclusion and exclusion criteria are shown Table 1.
The inclusion and exclusionc riteria
|
The inclusion criteria |
|
Patients over 18 years of age ASA 1-2 Patients did not have a mental or neurological disease Patients have no contraindications to ropivacaine and the drugs used in the study Patients agreed to cooperate in the study |
|
The exclusion criteria |
|
Patients with preoperative hemodynamic and respiratory disorders Patients with infection at the needle puncture site Patients with history of complications of surgery or anesthesia |
The patients were divided into two groups: group T received trigeminal (V) nerve block using ropivacaine under ultrasound guidance; and group C, the control group, received paracetamol infusion. Single-blinded randomization was conducted as follows: two tickets were numbered with either 1 or 2. If the first patient, picked number 1, that patient was included in group T; if the number was 2, the patient was enrolled in group C. The following patients were assigned, alternatively, such that the N patient was in group T, the N+1 patient was in group C, until the desired sample size was reached.
Protocols
To reduce the risk of nausea and vomiting, both groups of patients received intramuscular injections of 4 mg of dexamethasone and 8 mg of ondansetron prior to surgery. The induction was followed by fentanyl, 2 µg/kg; propofol, 2.5 mg/kg; and rocuronium bromide, 0.6 mg/kg. Maintenance of anesthesia included 2% sevoflurane; minimum alveolar concentration (0.8-1.2); fentanyl (repeat), 1 mcg/kg before skin incision; and Esmeron, 0.2 mg/kg if the surgery lasted for more than one hour. Cessation of anesthesia was carried out in Group T at the end of the surgery, after closure of the skin. Before extubation, 2 mL of 0.3% ropivacaine was injected at each site under ultrasound guidance to block the nerve branch V2 or V3, depending on the patient's skin incision site. Gas anesthesia was discontinued, the incision was bandaged, and the patient was transferred to the recovery room.
Interventions
Localized (nerve-block) anesthesia of the lower jaw was performed as follows. The probe was placed below the zygomatic arch, opposite the maxillary bone, and parallel to the zygomatic arch. Ultrasound imaging depicted the maxillary artery. A needle puncture was performed using the following method: the needle was directed perpendicularly to the probe (out of plane) and placed above the cheekbone arc with the needle tip located in the mandibular pterygium to avoid the maxillary artery, followed by aspiration. If no bleeding was observed, 0.5 mL saline was injected, and the fluid around the needle tip was assessed. If no bleeding was observed after aspirating, then 2 mL of local anesthetic was injected, while pausing to check every 1 mL to evaluate the image of local anesthetic distributed deep at the base of the mandibular pterygium. If both sides were numb, the other side was treated in the same manner.
For nerve anesthesia of the upper jaw, the probe was placed below the cheekbone after identifying the mandibular pterygium and moving the probe to the midface region. The goal was to inject local anesthetic into the palatine fossa, and to observe the tubercles of the maxillary bone, the lateral side of the pterygoid process, and the palatal foramen. Needle puncture was performed using the following method: the needle was placed perpendicular to the axis of the ultrasound beam, in which the role of the ultrasound was to determine whether the drug had been injected into the base of the palatine fossa. With the zygomatic arch technique, ultrasonography increases the success rate by showing the deep distribution of local anesthetic at the base of the palatal fossa. When the needle tip was in the palatine fossa and there was no blood with reaspiration, 0.5 mL of saline was injected and the liquid around the needle tip was observed. If there was no blood, 2 mL of local anesthetic was injected. Subsequently, the injection was stopped, and checked every 1 mL to visualize the deep distribution of anesthetic in the palatine fossa. If both sides were numb, the other side was treated in a similar fashion.
Group C was processed as follows: at the end of surgery, the skin was closed, the anesthetic was turned off, and the patient was moved to the recovery room. Before extubation, 1 g of paracetamol was infused intravenously at a rate of 100 drops/min.
After the block was completed, patients were monitored for pulse rate, blood pressure, respiratory rate, and SpO. Muscle relaxants were discontinued, and the endotracheal tube was extubated when all criteria were met, including being awake, performing simple movements as required, demonstrating a cough reflex and swallowing, no signs of dyspnea or respiratory disorders, a respiratory rate greater than 12 and less than 35 breaths per minute, and hemodynamic stability. The patient was monitored in the recovery room, evaluated according to the Aldrete scorecard, and transferred to the odontostomatology department.
Data from the study were collected during the first 24 hours after surgery. After 24 hours, patients were treated and cared for according to normal hospital routine. Both groups were monitored equally in the recovery room for pain score, visual analog scale (VAS) score, respiratory rate, SpO, pulse, and blood pressure. When the VAS score was ≥ 4, pain relief was provided by slow intravenous injection of 30 mg of ketorolac in 30 s. Pain was assessed 30 min after the injection was completed. If the VAS score was ≥ 4, 2 mg morphine was injected until VAS was < 4, with the total dosage not exceeding 10 mg (i.e., no more than 5 injections). During the titration of morphine, it was necessary to closely monitor pulse, blood pressure, respiratory rate, and SpO. Side effects were also monitored, detected, and treated.
Within the first 24 hours after surgery, several parameters were monitored, including the time required for the first dose of pain relief, 24-hour dose of ketorolac in both groups, VAS score at pre-determined timepoints (0, 1, 2, 3, 4, 6, 9, 12, 18, 24 hours after surgery), the patient at rest (when lying still and breathing normally without exertion), and when moving (changing position, turning the head, taking deep breaths, or opening the mouth to chew). Changes in circulation, including pulse rate, systolic blood pressure, diastolic blood pressure, and changes in respiration, including respiratory rate and SpO, were recorded. Systemic complications such as allergies, anaphylaxis, drug overdose, and anesthetic toxicity, as well as local complications such as vascular puncture, nerve damage, hematoma at the injection site, facial paralysis, jaw dropping, and paresthesia/numbness of the lips and tongue were also evaluated.
The data were analyzed using SPSS software (version 20.0). The results are described as mean ± standard deviation. Comparison of two values in the same group was calculated by t-test, and that in the two groups by ANOVA. Statistical significance was set at p < 0.05.

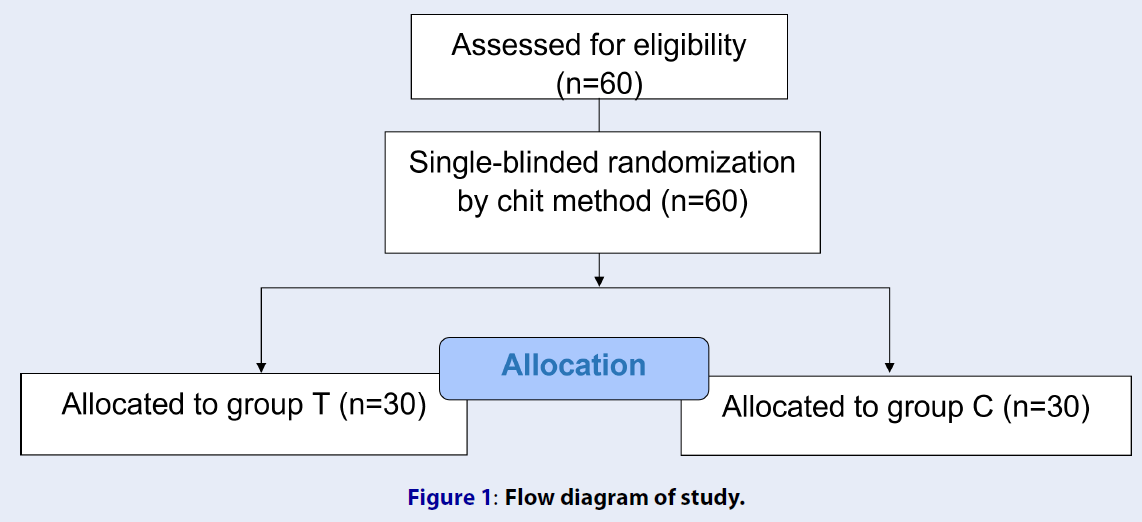
Flow diagram of study.
The baseline parameters of patients
|
Parameters |
Group T |
Group C |
p value |
|---|---|---|---|
|
Age (years) |
29.67 ± 11.46 |
29.17 ± 6.26 |
> 0.05 |
|
ASA |
> 0.05 | ||
|
I |
25 |
28 | |
|
II |
5 |
2 | |
|
Type of surgery | |||
|
Teeth removal |
16 |
18 |
0.47 |
|
Bone tumor dissection |
10 |
6 | |
|
Bone surgery |
4 |
6 | |
|
Surgery time (min) |
53.83 ± 17.06 |
55.07 ± 27.25 |
0.83 |
|
Used medicine | |||
|
Fentanyl (mg) |
0.20 ± 0.05 |
0.19 ± 0.04 |
0.39 |
|
Rocuronium bromide (mg) |
33.17 ± 5.00 |
33.00 ± 4.66 |
0.94 |
|
Propofol (mg) |
133.33 ± 35.07 |
130 ± 20.68 |
0.95 |
|
Number of incision | |||
|
1 |
12 |
14 |
0.72 |
|
2 |
3 |
5 | |
|
3 |
2 |
1 | |
|
4 |
13 |
10 |
The adverse effects ofboth groups
|
Time point |
Group T (number of patients) |
Group C (number of patients) | ||||
|
ausea |
Vomit |
Itching |
ausea |
Vomit |
Itching | |
|
H0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
H1 |
3 |
1 |
0 |
7 |
2 |
1 |
|
H2 |
0 |
0 |
0 |
1 |
1 |
0 |
|
H3 |
1 |
0 |
0 |
1 |
0 |
0 |
|
H6 |
1 |
1 |
0 |
2 |
1 |
0 |
|
H9 |
1 |
0 |
0 |
0 |
0 |
0 |
|
H12 |
0 |
0 |
0 |
0 |
0 |
0 |
|
H18 |
0 |
0 |
0 |
0 |
0 |
0 |
|
H24 |
0 |
0 |
0 |
0 |
0 |
0 |
Post-operative pain management
|
Parameters |
Group T |
Group C |
p value |
|---|---|---|---|
|
Starting time for pain killer (hours) |
7.63 ± 1.99 |
3.83 ± 1.29 |
< 0.01 |
|
Amount of Ketorolac (mg) |
35.17 ± 11.53 |
62.00 ± 7.61 |
< 0.01 |
Pain measurement after the surgery
|
Time point |
VAS at resting time (score) |
VAS at moving time (score) | ||
|
Group T |
Group C |
Group T |
Group C | |
|
H0 |
0 |
0 |
0 |
0 |
|
H1 |
2.07 ± 0.25* |
2.1 ± 0.31 |
2.10 ± 0.31* |
3.03 ± 0.18 |
|
H2 |
2.60 ± 0.53* |
3.0 ± 0.26 |
2.87 ± 0.63* |
3.60 ± 0.56 |
|
H3 |
3.15 ± 0.95* |
3.73 ± 0.83 |
3.30 ± 0.65* |
4.73 ± 0.83 |
|
H6 |
3.32 ± 0.68 |
3.3 ± 0.53 |
3.80 ± 1.03 |
3.80 ± 0.92 |
|
H9 |
3.18 ± 0.43 |
3.03 ± 0.18 |
4.03 ± 0.85 |
3.70 ± 0.47 |
|
H12 |
3.73 ± 0.73 |
3.90 ± 0.71 |
4.23 ± 0.94 |
4.56 ± 0.73 |
|
H18 |
3.30 ± 0.60 |
3.40 ± 0.67 |
3.63 ± 0.67 |
4.07 ± 0.98 |
|
H24 |
3.43 ± 0.57 |
3.23 ± 0.43 |
3.97 ± 0.49 |
3.83 ± 0.53 |
Results
Patient descriptions
The study included 60 patients (Figure 1), with a higher proportion of men, although the difference was not statistically significant (p > 0.05). The number of patients with comorbidities was higher in group T than in group C. Based on ASA physical status classification, most subjects had ASA I; this rate was lower in group T than in group C (83.3% and 93.3%, respectively), but the difference between the two groups was not statistically significant (p > 0.05, Table 2).
With regard to surgery type, patients in the two groups were primarily undergoing tooth extraction, and the number of patients undergoing this procedure in group C (18 patients) was higher than that in group T (16 patients). Other types of interventions included bone surgery, which was carried out in a similar number of patients in the two groups. Between the two groups, the patients’ surgical procedures had similar durations: 53.83 ± 17.06 min for group T and 55.07 ± 27.25 min for group C.
Side effects/adverse effects
Changes in hemodynamics and respiration were within normal limits throughout the study period. Adverse effects were reported in the first 9 hours after surgery and include nausea, vomiting, and itching (Table 3). The number of patients with nausea in group T (6 patients) was lower than that in group C (11 patients). Vomiting was reported in 2 patients in group T, and 4 patients in group C. No patients in group T, and 2 patients in group C reported itching. No bleeding, anesthetic toxicity, or pain medication overdose were reported.
During the nerve-block procedure in one patient, the needle was inserted into the blood vessel. After drawing out blood, the needle was withdrawn, pressure was applied to the point of bleeding for 3 minutes, and the needle puncture position redetermined prior to the administration of anesthetic. In group T, the patient had numbness of the lips and tongue, but it was still tolerable. No cases of facial paralysis were recorded.
Treatment efficacy
The time required for the first analgesic dose was 7.63 ± 1.99 h (3-10 h) in group T, and 3.83 ± 1.29 h in group C (2 - 6 h). In terms of the drug, the amount of ketorolac administered in group T was 35.17 ± 11.53 mg lower than that in group C (62.00 ± 7.61 mg, Table 4).
Resting VAS score increased over time in both groups but was lower in group T than in group C for the majority of timepoints. At H and H, a significant difference between the two groups was observed (p < 0.05). Moving VAS scores also increased over time in both groups. At H, H, and H, the VAS score of group T was significantly lower than that of group C (Table 5).
Discussion
The study was conducted in two groups of 30 patients each. All patients were randomly assigned and received the same anesthetic treatment to limit the influence of factors related to both operative and postoperative procedures.
The time period for the first dose of an analgesic was defined as the time from extubation until the patient felt pain with a VAS score ≥ 4, which is possibly comparable to the duration of the first dose of analgesics. We observed that the time period before the first dose of analgesics in group T (7.63 ± 1.99 h) was longer than that in group C (p < 0.01). Under the guidance of ultrasound, the position of the nerve could be determined with greater accuracy, leading to an improved technique that enabled the anesthetic to be concentrated at the numbing site. In a study by Ducan et al. (2013)6, anesthesia was administered to two groups (60 patients) using a nerve stimulator and ultrasound, with a duration of anesthesia in the ultrasound group of 429.5 minutes (7.16 h).
With regard to the dosage of ketorolac, most of the cases in group C used more pain medication at the time of H2 and H3, while in group T, it was about 6 - 9 h after surgery. The dose of ketorolac in group T was 30 - 60 mg, whereas in group C it was 60 ‑ 90 mg (p < 0.05). This finding suggests that paracetamol 1 g/100 mL intravenous injection alone was not sufficient in some patients, who required additional analgesics or another method of pain relief.
In our study, the pain level in patients after maxillofacial surgery was mainly mild or moderate depending on the surgical technique and the patient’s characteristics. Resting VAS was lower in group T than in group C at most timepoints. However, only at time H2 and H3, was the difference between the two groups statistically significant (p < 0.05). Active VAS increased over time in both groups, but was lower in group T than in group C at most timepoints. At time H1, H2, and H3, the difference between the two groups was statistically significant (p < 0.05). Our results are similar to those reported by Jain et al. (2016)7. The VAS score in the group using the V2 and V3 nerve anesthesia method under ultrasound guidance was lower than that of the other group, but higher than that found in our study (3.12 ± 3.04 vs. 4.61 ± 4.45)7. In a study by Bouzinac et al., the local anesthetic ropivacaine was used, resulting in a low pain level with VAS ≤ 2 at 4, 8, 12, 16, 20, and 24 h post-surgery8. The pain-relief effect of this method lasted longer than our approach because the authors used an additional intravenous infusion of 1 g of paracetamol and an intravenous injection of 50 mg ketoprofen every 6 h and 12 h8. We found that the duration of pain relief for the paracetamol infusion group was only effective approximately 4 h after surgery. For the group receiving V nerve anesthesia under ultrasound guidance, the pain levels were mild, with the analgesic still in effect at 6 h after surgery.
In this study, we also noted the postoperative adverse effects of nausea, vomiting, itching, and bleeding. Maxillofacial surgery directly interferes with the upper respiratory tract. After surgery, if the surgeon does not remove all the fluid and blood from the nose and pharynx, the patient is susceptible to aspiration after extubation. In the postoperative period, the overall incidence of nausea and vomiting in all types of surgery and in different populations varied between 25% and 30%. However, the rate of persistent and difficult vomiting accounted for 0.18% of the total number of patients9. Based on these preliminary results, it can be inferred that V nerve block anesthesia under ultrasound guidance for large and complex surgeries in the maxillofacial region is appropriate. However, the nerve-blocking agent can only be injected once, so it is preferable to combine dexamethasone with the local anesthetic ropivacaine to prolong the duration of postoperative analgesia.
Despite the promising results of this study, some limitations should be taken into consideration, including small sample size and heterogeneous types of surgery, such that the pain level was not the same across procedures. In addition, the surgeries described in this study typically result in a low level of pain, so the differences were not large compared to the intravenous analgesia group. In major maxillofacial surgeries that require cutting into the jawbone or repairing the large jawbone due to trauma, the use of regional anesthesia can be clearly effective. Another limitation is that the study was not able to follow up patients for a long period of time after surgery, so we were unable to assess the reduction in chronic pain. Chronic pain can persist up to 6 months after surgery, which could have a substantial effect on the quality of life of patients.
Conclusions
This study enrolled 60 patients who underwent maxillofacial surgery. The initial evaluation showed that the method of V2 and V3 nerve block under ultrasound guidance provided increased pain relief compared to intravenous paracetamol. The VAS score in the study group was lower than that of the control group at most timepoints assessed. However, only at the second and third postoperative hour was the difference between the two groups statistically significant. Group T tolerated a later first dose of analgesic with a lower dose of ketorolac. In both groups, the patient’s respiration and circulation fluctuated, but remained within the normal range. In the anesthesia group, all patients had minor numbness of the lips and tongue, no facial paralysis, and no hematoma. The rates of nausea, vomiting, and itching in the two groups did not differ, and no bleeding, anesthetic toxicity, or analgesic overdose were recorded. Overall, this intervention could enhance patient satisfaction, and the procedure has potential as an effective pain management technique in maxillofacial surgery.
Abbreviations
ASA: American Society of Anesthesiologists; H: Time after 2,3,4,… hours; NSAIDs: Non-steroidal anti-inflammatory drugs; SpOSaturation of peripheral oxygen; VAS: visual analog scale
Acknowledgments
None.
Author’s contributions
Quang Minh Pham: Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing; Duong Thi Bach Nguyen: Investigation, Methodology, Data analysis; Anh Xuan Nguyen: Investigation, Methodology, Data analysis; Phuong Thi Thu Tran: Data analysis, Writing – original draft, Writing – review & editing. All authors read and approved the final manuscript.
Funding
None.
Availability of data and materials
Data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
This study was conducted in accordance with the amended Declaration of Helsinki. Ethical permission for this study was obtained from the ethics committee of Thai Nguyen Medical University (Number: 239/ĐHYD-HĐĐĐ).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.